Histopathology aiding diagnosis of viscerocutaneous loxoscelism in a nonendemic region
Smrithi Mani, Charles Katzman, Vincent Liu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
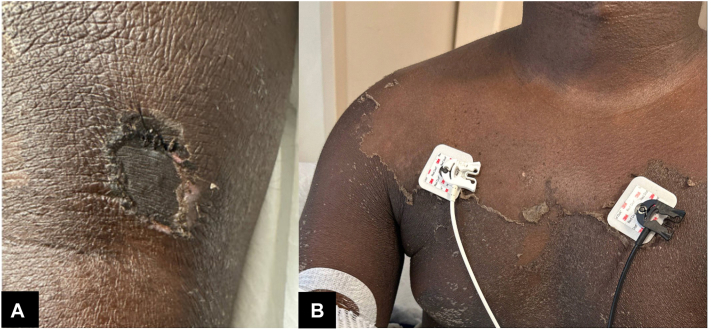 Figure 1
Figure 1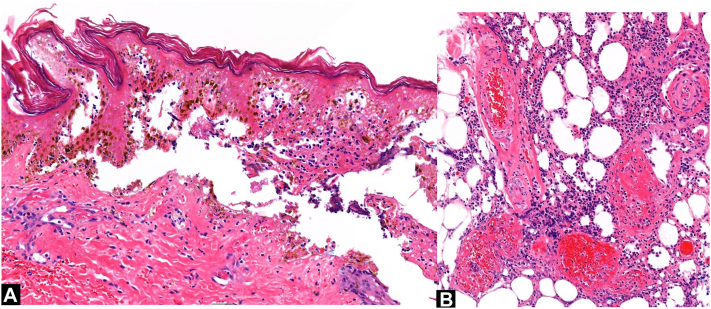 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVector-borne infectious diseases · Venomous Animal Envenomation and Studies · Bartonella species infections research
Introduction
Viscerocutaneous loxoscelism is a rare syndrome caused by brown recluse spider envenomation.1 In addition to the cutaneous manifestation of a necrotic wound, it can present with systemic symptoms, including acute hemolytic anemia, renal failure, disseminated intravascular coagulopathy, and even death.1, 2, 3 The Loxosceles reclusa is responsible for most cases of loxoscelism in the United States.2 Diagnosis and management of viscerocutaneous loxoscelism can pose challenges because of the often undetected initial bite and limited studies on treatment.3 We report a delayed diagnosis of fulminant viscerocutaneous loxoscelism in a nonendemic region supported by histopathology.
Case report
A previously healthy 19-year-old Black man was transferred to our intensive care unit for an acute drop in hemoglobin. In the week before admission, the patient presented to his local emergency department for fever, malaise, and vomiting. A lesion behind his left knee was noted, initially considered unrelated and benign. He was diagnosed with a viral illness and sent home. The day before transfer, he returned to the emergency department for worsening symptoms and a syncopal episode. The lesion behind his knee had become tender and swollen. Computed tomography of the left lower extremity was consistent with cellulitis. Given clinical concern for sepsis, he received clindamycin before his hemoglobin dropped to 3.4 g/dL. He was stabilized with 2 units of packed red blood cells and transferred.
Admission laboratory results showed hemolytic anemia. Etiology was unknown at the time. The patient received intravenous immunoglobulin and dexamethasone while the hematology and infectious disease services conducted their investigations. During initial hospitalization, he experienced significant respiratory distress secondary to pulmonary edema, gross hematuria, and laboratory studies showed transaminitis, leukocytosis, and significantly elevated inflammatory markers (Table I).Table ILongitudinal laboratory values, important events, and workup during hospitalizationLaboratory tests∗Hospital day12345678Blood count White blood cell count (K/mm^3^)33.3741.739.139.1, 43.232.717.112.68.7 Hemoglobin (g/dL)3.4, 4.1, 6.56.0, 7.3, 7.07.06.9, 9.18.48.98.48.8 Platelets (K/mm^3^)165--69585359-Hemolysis laboratory results Total bilirubin (mg/dL)14.54.41.9--1.31.21.1 PT/INR (s/IU)13/1.2------- Lactate dehydrogenase (μ/L)1601----767599- # Reticulocyte count (K/mm^3^)48.0----390.9-- Haptoglobin (mg/dL)<10----<101331 Kidney/liver function AST (μ/L)45, 14214445--292225 ALT (μ/L)30, 10710768--574947 BUN (mg/dL)2421202120181615 Creatinine (mg/dL)1.080.860.920.910.900.900.860.83Important eventsDiffuse desquamating rash; pulmonary edemaSeizure-like episodeTreatmentIVIG (1 g/kg, 2 doses), 2 units of PRBCs, solumedrol, dexamethasone (40 mg, 4 doses), levetiracetam (started on day 4), several antibiotic courses (clindamycin, doxycycline, ceftriaxone, metronidazole, vancomycin)**Workup for alternateetiologies (allinsignificant)Anaplasma phagocytophilum (Ab and PCR); Ehrlichia chaffeensis, Ehrlichia ewingii, Ehrlichia muris-like (Ab and PCR); Lyme disease (Ab); MRSA; blood culture, Staphylococcus aureus PCR, Legionella antigen, acid-fast bacilli culture, fungal culture, Giemsa stain, Malaria panel, Histoplasma antigen, Blastomyces antigen, Syphilis Ab, HIV (Antigen/Ab and PCR), Chlamydia PCR, Gonorrhea PCR, Hepatitis A/B/C Ab, EBV Ab, CMV PCR, Cardiolipin Ab, ANCA, ANA, Antistreptolysin, DNase B Ab, ADAMTS-13, Copper, Folate, B12Ab, Antibody; ALT, alanine transaminase; AST, aspartate transaminase; BUN, blood urea nitrogen; EBV, Epstein-Barr virus; IVIG, intravenous immunoglobulin; PCR, polymerase chain reaction; PRBCs, packed red blood cells, PT/INR, prothrombin time/international normalized ratio.∗Normal ranges: white blood cell (3.5-10.5), hemoglobin (13.2-17.7), platelets (150-400), total bilirubin (<1.2), PT (9-12), INR (<4.0), lactate dehydrogenase (135-225), # reticulocyte (12.0-130.0), haptoglobin (30-200), AST (0-40), ALT (0-41), BUN (10-20), creatinine (0.67-1.17).
On day 2 of hospitalization, a widespread desquamating rash developed on his trunk, face, and extremities. Dermatology was consulted for the rash and the lesion in the left popliteal fossa (Fig 1). On interview, the patient had noted a “scratch” in the left popliteal area 1 week before hospitalization, which was itchy but not painful. He did not recall a definite spider bite but mentioned noticing spiders in their home in Iowa and sleeping on a floor mattress. The lesion had developed into a depressed, ulceronecrotic, atrophic, hyperpigmented plaque with scalloped borders, eschar formation, and surrounding induration.Fig 1A, Necrotic eschar in the left popliteal fossa. B, Diffuse desquamation of the chest.
After our interview and physical examination, we obtained a single punch biopsy from the superomedial edge of the eschar. Histopathologic examination of the biopsy showed epidermal necrosis, superficial and deep neutrophilic vasculitis with vessel wall destruction, fibrin deposition, and karyorrhectic debris surrounding the dermal vessels (Fig 2). Special histochemical stains for acid fast, Gram, and periodic acid–Schiff, as well as immunohistochemical stains for spirochetes, herpes simplex virus, and varicella-zoster virus were negative for microorganisms. Histopathologic changes were deemed compatible with venomous arthropod assault.Fig 2. Histopathology of skin biopsy of left popliteal eschar. A, Epidermal necrosis (hematoxylin-eosin stain; original magnification: ×400). B, Neutrophilic vasculitis of pannicular blood vessels (hematoxylin-eosin stain; original magnification: ×200).
The constellation of his unexplained symptoms with the necrotic appearing eschar, in conjunction with his laboratory and histopathologic data, was consistent with a diagnosis of viscerocutaneous loxoscelism. His diffuse skin sloughing was also attributed to loxoscelism.
Extensive workup for alternate etiologies was unrevealing (Table I). Direct Coombs testing was weakly positive. As his anemia improved, dexamethasone was discontinued. He experienced another syncopal episode, but all neurologic and cardiac workup was unremarkable. Ultimately, on hospital day 8, he was discharged.
Discussion
We present this case of a previously healthy 19-year-old Black man with dermatologic findings of a necrotic eschar and widespread desquamating rash and systemic findings of acute hemolytic anemia, transaminitis, and pulmonary edema. Our patient’s florid systemic reaction, constellation of cutaneous findings, striking laboratory data, clinicopathologic correlation, and unusual geographic exposure history expands our appreciation of the presentation spectrum of viscerocutaneous loxoscelism. Although our patient could not provide physical evidence of a brown recluse spider from his home, the pattern and timing of his clinical symptoms coupled with the negative workup for alternate etiologies favor the diagnosis of viscerocutaneous loxoscelism over other infectious, autoimmune, or neoplastic causes (Table I).
Definitive diagnosis of loxoscelism requires confirmation of a bite and patient presentation of the offending spider for identification1; however, these criteria are not met in approximately 90% of suspected spider bite cases.2 Although there is an enzyme-linked immunosorbent assay available to detect Loxosceles venom, it is not commercially available and is primarily for research.4 Therefore, the primary suspicion for loxoscelism usually derives from report of a sensation of a possible bite. In about 40% of loxoscelism cases, including ours, there is no definite reported bite.1 An initial bite may go unnoticed, as it is fairly painless and commonly occurs at night.1, 2, 3
Given the elusive nature of diagnostic confirmation of loxoscelism, our case uniquely features the value of histopathologic data in corroborating a loxoscelism diagnosis, which is more accessible than enzyme-linked immunosorbent assay testing and provides a more conclusive assessment beyond clinical suspicion alone. Our histologic findings favor brown recluse envenomation over alternative arthropod assault because of the neutrophilic vasculitis, consistent with the study of 41 skin histologic specimens from rabbits injected with brown recluse spider venom.5 Histologic sampling from the rabbit wound site consistently showed epidermal and dermal necrosis, surrounding mixed inflammatory infiltrate with neutrophils, and small vessel vasculitis, aligning with our findings.5
L reclusa’s native range historically encompasses central and southeastern states.2 Awareness of this range aids in early detection for patients within endemic regions and helps to avoid potential misdiagnoses in nonendemic areas.2 However, our patient whose exposure in a nonendemic area which primarily lies outside the native region, highlights the importance of caution in reliance of geographic exposure, and underscores the critical utility of familiarity with the clinical features of loxoscelism for physicians.2 The diagnosis of viscerocutaneous loxoscelism in the state of Iowa is exceptionally rare, with the last published case being in 1980.6
Our patient had a particularly severe case of systemic loxoscelism, with his hemoglobin reaching a nadir of 3.4. The primary team was uncertain about the etiology of his anemia, possibly because of the infrequency of loxoscelism in nonendemic regions or challenges in identifying the cutaneous manifestations in individuals with darker skin tones. However, the dermatology team successfully diagnosed the condition by observing the eschar and widespread skin desquamation. This distinct cutaneous pattern associated with loxoscelism has previously been described in other patients with skin of color.7^,^8 Acute generalized exanthematous pustulosis has been reported as another diffuse rash associated with loxoscelism.9
Diagnosis of viscerocutaneous of loxoscelism can be useful to avoid unnecessary treatment for the many mimics including infection, necrotizing vasculitides, and neoplastic disease.9 Treatment of loxoscelism is controversial given cutaneous and systemic symptoms should resolve on their own.1^,^3^,^9 Various approaches have been trialed, but their effectiveness is inconclusive.1, 2, 3^,^9 Supportive care is the general recommendation in North America.3
Autoimmune hemolytic anemia is the characteristic feature of viscerocutaneous loxoscelism.1, 2, 3 Other systemic manifestations are relatively heterogenous but include neurologic symptoms, transaminitis, and pulmonary edema our patient experienced (Table II).10 Loxosceles spider venom contains an array of protein factors that contribute to the cutaneous and systemic manifestations of loxoscelism including hyaluronidase, alkaline phosphatase, esterase, ATPase, and sphingomyelinase D.3 Sphingomyelinase D, the predominant toxic enzyme, hydrolyzes sphingomyelin found in cell membranes, contributing to both dermonecrosis and hemolysis of red blood cells.3Table IICases of viscerocutaneous loxoscelism in the United States∗StudyPatientRaceStateDiagnosisTreatment†AbxDermatologic features‡Clinical features§Edwards et al661 MCIAClinicalSteroidsYGangrene of eyelidsSevere laryngeal edema with upper airway obstruction, seizuresCain et al1125 M-KSClinicalSteroids, plasma exchangeY-ICU transferAbraham et al1217 F-KSClinicalSteroids, plasma exchangeY-ICU transferDiPaola et al1319 MCKYClinicalSteroidsY-Rhabdomyolysis, acute kidney injury, transaminitisLangner et al1016 MBMOELISA for Loxosceles reclusa venomSteroids, IVIG, plasmapheresisN-Myocarditis, pulmonary edema, cardiogenic shock, hypotension requiring ICU care, DIC, transaminitisMueller et al925 FSAMOClinicalSteroids, IVIGYAGEP with extensive desquamationTransaminitis, ICU care for severity of anemiaNeverman et al1416 MBMOClinical-Y-TransaminitisHarry et al1549 MCMOClinicalPlasmapheresisY-Renal failure requiring hemodialysis, transaminitisCalhoun et al1630 M, 28 FBMOClinicalSteroidsY-Transaminitis, acute kidney injury, spontaneous abortionSchmid et al724 FBMOClinical-YDiffuse desquamating rashPleural effusion, pericardial effusion, cANCA/antiprotease-3 vasculitisSchilli et al1779 MCMOELISA for L reclusa venomSteroidsY-Obtundation, syncope, myocardial infarctionAnwar et al1820 MBMOClinicalSteroids, IVIGYAGEPHypoxic respiratory failure, transaminitis, pancreatitis, cardiomyopathy, ICU transferLane et al199 MBMOClinical (spider available)-NAGEPTransaminitis, ICU transfer, high output heart failure, respiratory distressStoecker et al2016 M-MOELISA for L reclusa venomSteroidsN-TransaminitisKodali et al2134, 31, 21, 21, 25, 22-MOClinical-N“Diffuse rash”Hepatosplenomegaly, syncope, necrotizing fasciitis, hypotensive shock requiring ICU careLane et al2219 F, 9 FBMOClinicalSteroidsY--Said et al236 MBMOClinicalPlasma exchangeN-DIC, renal failure, hypotensive shock requiring ICU careZimmerman et al2412 F, 9 FBNCClinical (spider available)SteroidsYScarlatiniform rashPulmonary edema, toxic shock syndromeDandoy et al2510 MBTNClinicalSteroidsN-HLH, splenomegaly, transaminitis, renal failure requiring hemodialysisRosen et al263 MCTNClinical-N-DeathMcDade et al2717 F, 16 M, 13 M, 12 F, 13 F, 14 FBTNClinical-NDesquamation surrounding necrotic woundSevere hypotension requiring ICU careDonepudi et al811 MBTNClinical-YDesquamating, depigmenting rash on face, neck, and trunk-Elbahlawan et al2815 M, 15 F, 3 M, 12 M, 10 M, 11 MBTNClinicalDapsone, steroidsYDiffuse desquamating rashPulmonary edema, renal failure requiring hemodialysis, severe hypotension, ICU transferWilliams et al2926 F, 17 FBTNClinicalSteroidsYFine papular rash of the extremities, extensive skin sloughing extending from necrotic woundDeath, pulmonary edema, pleural effusion, pericardial effusion, hepatic congestionRogers et al3011 MCTNClinical-Y-ICU transferMichaud et al316 MC/KTNClinical-NDiffuse erythematous, pruritic macular rash with petechiae-Hogan et al3211 MBTNClinicalSteroidsYTiny papules from umbilicus spreading outwardRobb et al3349 F-TNClinical (spider available)Steroids, dapsoneNSunburn-like, purpuric eruptionWilson et al3424 FCTXClinical (spider available)Dapsone, steroids, hyperbaric oxygen therapyNFine macular rash over trunk and extremities-Goto et al357 M-TXClinical (spider available)Steroids, dapsoneY-Upper airway obstruction secondary to edema, ICU transferAbx, Antibiotics; AGEP, acute generalized exanthematous pustulosis; B, Black; C, Caucasian; DIC, disseminated intravascular coagulation; ELISA, enzyme-linked immunosorbent assay; F, female; IA, Iowa; ICU, intensive care unit; IVIG, intravenous immunoglobulin; K, Korean; KS, Kansas; KY, Kentucky; M, male; MO, Missouri; N, no; TN, Tennessee; TX, Texas; Y, yes.∗This table includes case reports and series from the United States based on search of “systemic loxoscelism” and “viscerocutaneous loxoscelism” on PubMed, EMBASE, and Cochrane databases. Studies that were retrospective reviews, abstracts only, or did not have full text were not included.†Treatment does not include supportive measures such as fluid resuscitation or blood transfusion.‡Dermatologic features do not include necrotic wound itself.§Clinical features do not include hemolysis or nonspecific constitutional symptoms. Of note, 78% (29/37) of patients in case reports with data on race were Black.
Viscerocutaneous loxoscelism can be a difficult diagnosis, especially in a nonendemic region where there is no reported bite and symptoms resemble more common disease processes. We highlight specific cutaneous and histopathologic features to aid in this challenging diagnosis.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Isbister G.K.Fan H.W.Spider bite Lancet 378980820112039204710.1016/s 0140-6736(10)62230-121762981 · doi ↗ · pubmed ↗
- 2Swanson D.L.Vetter R.S.Bites of brown recluse spiders and suspected necrotic arachnidism N Engl J Med 3527200570070710.1056/NEJ Mra 04118415716564 · doi ↗ · pubmed ↗
- 3Swanson D.L.Vetter R.S.Loxoscelism Clin Dermatol 243200621322110.1016/j.clindermatol.2005.11.00616714202 · doi ↗ · pubmed ↗
- 4Stoecker W.V.Green J.A.Gomez H.F.Diagnosis of loxoscelism in a child confirmed with an enzyme-linked immunosorbent assay and noninvasive tissue sampling J Am Acad Dermatol 555200688889010.1016/j.jaad.2006.04.06517052500 PMC 3196352 · doi ↗ · pubmed ↗
- 5Elston D.M.Eggers J.S.Schmidt W.E.Histological findings after brown recluse spider envenomation Am J Dermatopathol 223200024224610.1097/00000372-200006000-0000610871067 · doi ↗ · pubmed ↗
- 6Edwards J.J.Anderson R.L.Wood J.R.Loxoscelism of the eyelids Arch Ophthalmol 981119801997200010.1001/archopht.1980.010200408490127436834 · doi ↗ · pubmed ↗
- 7Schmid K.M.Treaster M.R.Barrios C.Zhang C.Scalzo A.J.Heightened immune response to presumed Loxosceles reclusa envenomation Wilderness Environ Med 304201945045310.1016/j.wem.2019.06.01431685322 · doi ↗ · pubmed ↗
- 8Donepudi S.K.Ahmed K.A.Stocks R.M.Nelson D.Thompson J.W.Aural involvement in loxoscelism: case report and literature review Int J Pediatr Otorhinolaryngol 691120051559156110.1016/j.ijporl.2005.04.01515939487 · doi ↗ · pubmed ↗