Rapid detection of Staphylococcus aureus in blood culture samples using human IgG-based lateral flow assay
Arpasiri Srisrattakarn, Nicha Charoensri, Jeerati Prompipak, Wajeeorn Ouancharee, Bhanubong Saiboonjan, Patcharaporn Tippayawat, Aroonwadee Chanawong, Lumyai Wonglakorn, Ekgarak Kanwattanee, Sirikan Piyapatthanakul, Thitimar Masmalai, Anisara Ariyapim, Rinjong Promson Kendal

TL;DR
A new rapid test using human IgG detects Staphylococcus aureus in blood samples within 15 minutes, potentially enabling faster diagnosis and treatment.
Contribution
The study introduces a cost-effective lateral flow immunoassay using human IgG for S. aureus detection, offering a faster alternative to traditional methods.
Findings
The LFIA achieved 100% sensitivity and 92.4%-100.0% specificity in spiked blood culture samples.
The detection limit for purified protein A was 10−3 µg/mL and for bacterial colonies was 107 CFU/mL.
The test showed 98.1% sensitivity in 221 bacterial colony isolates and 89.7% in 118 positive blood culture bottles.
Abstract
Staphylococcus aureus is one of the most common pathogens. The conventional workflow for identifying this organism is time-consuming and takes up to several days. Therefore, we developed a colloidal gold-based lateral flow immunoassay (LFIA) using human IgG as a conjugated antibody to detect S. aureus. One hundred and thirty-eight clinical isolates, including 79 S. aureus and 59 non-S. aureus were spiked in blood samples, and incubated at 37°C for 24 h. The bacterial antigens were simply extracted before being tested by the developed LFIA strips. The results were read by the naked eye within 15 min. Conventional PCR was used as a reference method. The sensitivity and specificity of the developed LFIA were 100% (95% CI: 94.2%–100.0% and 92.4%–100.0%, respectively) in spiked blood culture samples. The detection limits of the LFIA for the purified protein A and bacterial colonies were 10−3…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
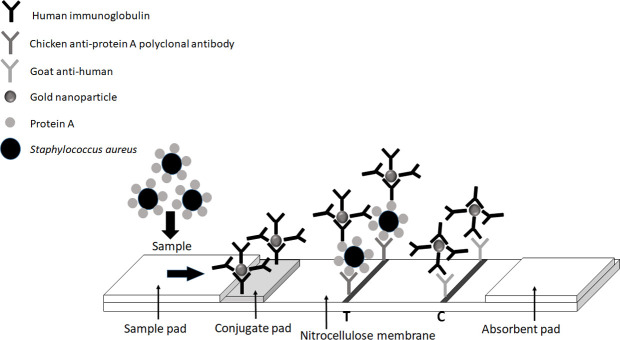 Fig 1
Fig 1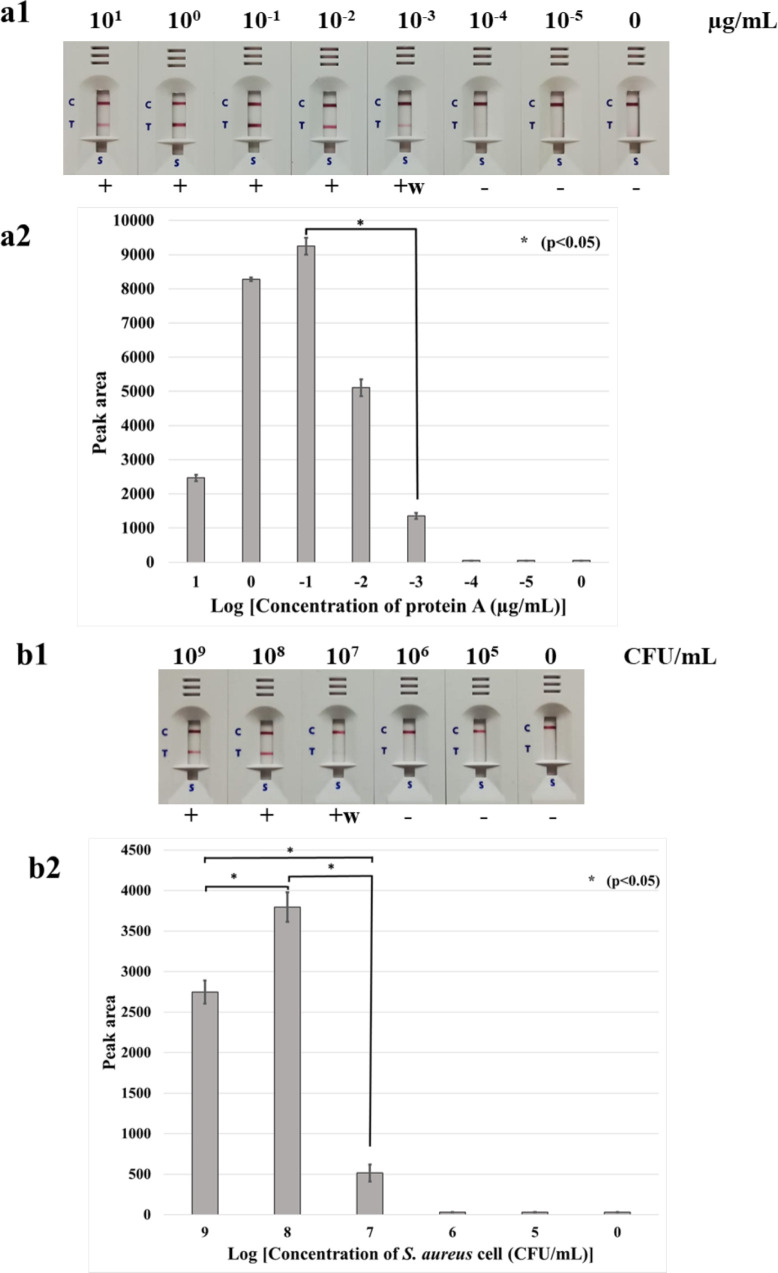 Fig 2
Fig 2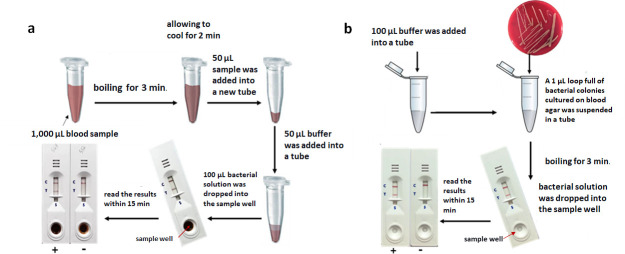 Fig 3
Fig 3| Pathogens ( | No. of isolates tested by | ||||
|---|---|---|---|---|---|
| PCR for | LFIA | ||||
| Positive | Negative | Positive | Weakly positive | Negative | |
| Gram-positive bacteria (126) | |||||
| | 79 | 0 | 68 | 11 | 0 |
| | 0 | 3 | 0 | 0 | 3 |
| | 0 | 2 | 0 | 0 | 2 |
| | 0 | 2 | 0 | 0 | 2 |
| | 0 | 2 | 0 | 0 | 2 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 12 | 0 | 0 | 12 |
| | 0 | 9 | 0 | 0 | 9 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 2 | 0 | 0 | 2 |
| | 0 | 2 | 0 | 0 | 2 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| Gram-negative bacteria (11) | |||||
| | 0 | 4 | 0 | 0 | 4 |
| | 0 | 3 | 0 | 0 | 3 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| Yeast (1) | |||||
| | 0 | 1 | 0 | 0 | 1 |
|
|
|
|
|
|
|
| Species ( | No. of isolates tested by | ||||
|---|---|---|---|---|---|
| PCR for | LFIA | ||||
| Positive | Negative | Positive | Weakly positive | Negative | |
| Bacterial colonies (221) | 160 | 61 | 151 | 6 | 64 |
| Hospital A (221) | |||||
| Gram-positive bacteria (195) | |||||
| | 160 | 0 | 151 | 6 | 3 |
| | 0 | 9 | 0 | 0 | 9 |
| | 0 | 9 | 0 | 0 | 9 |
| | 0 | 2 | 0 | 0 | 2 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 10 | 0 | 0 | 10 |
| | 0 | 3 | 0 | 0 | 3 |
| Gram-negative bacteria (26) | |||||
| | 0 | 8 | 0 | 0 | 8 |
| | 0 | 6 | 0 | 0 | 6 |
| | 0 | 5 | 0 | 0 | 5 |
| | 0 | 4 | 0 | 0 | 4 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| Positive blood cultures (118) | 68 | 50 | 58 | 3 | 57 |
| Hospital A (33) | |||||
| Gram-positive bacteria (27) | |||||
| | 15 | 0 | 12 | 0 | 3 |
| | 0 | 5 | 0 | 0 | 5 |
| | 0 | 3 | 0 | 0 | 3 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| Gram-negative bacteria (4) | |||||
| | 0 | 2 | 0 | 0 | 2 |
| | 0 | 2 | 0 | 0 | 2 |
| Yeast (1) | |||||
| | 0 | 1 | 0 | 0 | 1 |
| Mix Gram-positive bacteria and Yeast (1) | |||||
| | 0 | 1 | 0 | 0 | 1 |
| Hospital B (76) | |||||
| Gram-positive bacteria (65) | |||||
| | 50 | 0 | 44 | 3 | 3 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 2 | 0 | 0 | 2 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 2 | 0 | 0 | 2 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| Gram-negative bacteria (10) | |||||
| | 0 | 2 | 0 | 0 | 2 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
| Mix Gram-positive and negative bacteria (1) | |||||
| | 1 | 0 | 1 | 0 | 0 |
| Hospital C (9) | |||||
| Gram-positive bacteria (5) | |||||
| | 2 | 0 | 1 | 0 | 1 |
| | 0 | 2 | 0 | 0 | 2 |
| | 0 | 1 | 0 | 0 | 1 |
| Gram-negative bacteria (4) | |||||
| | 0 | 2 | 0 | 0 | 2 |
| | 0 | 1 | 0 | 0 | 1 |
| | 0 | 1 | 0 | 0 | 1 |
- —Khon Kaen University (KKU)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFood Industry and Aquatic Biology
INTRODUCTION
Staphylococcus aureus is an important bacterial pathogen in humans, causing various critical infectious diseases such as septicemia, toxic shock syndrome, pneumonia, and infective endocarditis (1, 2). S. aureus is one of the leading pathogens of bloodstream infections, the second rank to Escherichia coli. The hospital mortality rate for S. aureus bacteremia ranges from 15% to 40% (3). Delays in identifying sepsis increase mortality in advanced stages of severity or septic shock (4). Therefore, rapid identification and early treatment further decreased the number of severe cases and yearly deaths.
Various approaches for early identification of bacteria from a positive blood culture include Gram staining, conventional biochemical assay, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry, PCR, and nanoparticle probe technology. Gram staining is a useful tool to guide an empirical therapy before final culture results are available (5). However, the Gram staining method has wide variations in sensitivity and specificity. Conventional biochemical assays are time-consuming and labor-intensive. The other systems require specialized equipment and are not widely available, especially in poor-resource countries.
A colloidal gold-based lateral flow immunoassay (LFIA) is a rapid, easy-to-use, and inexpensive method. No instrumentation or experts are required. Generally, antibody-based LFAs require the screening process of paired antibodies [conjugate (capture) and detection antibodies] for the sandwich structure reaction, which is usually associated with a high cost of the antibodies. The Fc region of mammalian IgG can naturally conjugate with protein A on the cell surface of S. aureus (6). The LFIA technique has been applied to detect S. aureus by using a specific antibody (anti-protein A) as a conjugated antibody (7–9). However, human IgG has not yet been used as a conjugated antibody and applied to a fully clinical specimen from hospitals. Therefore, we developed the colloidal gold-based LFIA assay by using a human IgG as a conjugated antibody for the detection of S. aureus (Fig. 1), which makes the colloidal gold-based LFIA assay more cost-effective for the routine detection of S. aureus. We also evaluated the performance of the test in three hospitals.
Schematic description of LFIA system: The LFIA consists of the sample pad; the conjugate pad with gold nanoparticle-labeled human immunoglobulin; the nitrocellulose membrane with a test line (T) consisting of chicken anti-protein A polyclonal antibody; a control line (C) consisting of goat anti-human IgG antibody recognizing the gold nanoparticle-labeled human immunoglobulin; and the absorption pad.
RESULTS
The detection limit of the LFIA method
The detection limit was tested in triplicate. We found no significant difference between the triplicate tests (P = 0.24 and 0.06 for the testing with Protein A and bacterial cells, respectively). The comparison of the peak area of each concentration showed significant difference (P < 0.05). The present developed LFIA showed a detection limit of 10^−3^ µg/mL of purified protein A. The limit of the LFIA for the detection of S. aureus from the colony was 10^7^ CFU/mL (10^6^ CFU/reaction). A result due to the “hook” effect (10) of the LFIA test was found with 10^1^–10^0^ µg/mL of purified protein A and 10^9^ CFU/mL of bacterial colonies (Fig. 2).
The detection limit of the developed LFIA for detection of protein A in purified protein (101–10−5 µg/mL) (a1 and a2) and bacterial colonies (109–105 CFU/mL) (b1 and b2). For the detection limit of purified protein, the concentrations of purified protein A (Arista Biological) varied from 101 to 10−5 µg/mL. (a2 and b2) the bar graph representing the peak area of the test line responding from a1 and b1. For the detection limit of bacterial colonies, the bacterial suspension to a turbidity of 1.0 McFarland standard (3 × 108 CFU/mL) was serially 10-fold diluted and confirmed by plating on agar for determination of the CFU. With 101–100 µg/mL of purified protein A and 109 CFU/mL of bacterial colonies, the LFIA showed results due to the “hook” effect. C, control line; T, test line; +, positive result; +w, weakly positive (two red lines of both test and control lines); −, negative result (one red line of the control line only).
Detection of S. aureus using LFIA in spiked blood culture samples
Using the PCR as a gold standard method, the LFIA strip could detect all S. aureus isolates in spiked blood culture samples (sensitivity of 100%; 95% CI: 94.2%–100.0%) within 15 min (no significant difference between the results of the LFIA test and PCR method, P = 0.36–0.75 by using Z-test for independent proportion). Weakly positive results were seen in 11 of 79 S. aureus samples. The test also showed no false positive result (100% specificity; 95% CI: 92.4%–100.0%) (Table 1).
Evaluation of the LFIA for direct detection in bacterial colonies and positive blood culture bottles in three hospitals
Testing with the bacterial colonies, the LFIA failed to detect 3 of 160 S. aureus isolates. The results showed excellent sensitivity and specificity (98.1% and 100%; 95% CI: 94.1%–99.5% and 92.6%–100.0%, respectively). For evaluation in positive blood culture bottles from three hospitals, the LFIA gave 89.7% (95% CI: 79.3%–95.4%) sensitivity, 100% (95% CI: 91.1%–100.0%) specificity compared with those of the PCR method. There were 7 false-negative results from the 68 S. aureus-positive blood cultures (Table 2).
Stability of the LFIA strip
After storage for 6, 12, and 24 months, the developed LFIA strips still gave clearly positive results with 0.01 µg/mL of protein A without reduced sensitivity but slightly reduced the T-line intensity. The signal intensity stored at 10°C was higher than that of 25°C. These results indicated that the LFIA strips can be stored at 10°C for at least 24 months without losing their efficacy (see Fig. S1 at https://doi.org/10.6084/m9.figshare.24429058).
Whole-genome sequencing to compare the molecular characteristics of spa gene
Genome analysis of one representative with a false-negative result revealed that the spa gene is truncated with a stop codon (TAA) in the coding sequences (mutant strain). The spa gene was mutated by a novel C to T base substitution (C130T), resulting in a truncated protein A in comparison with the full-length spa gene of S. aureus N315 (a positive-strain; accession number: BA000018; see Fig. S2 at https://doi.org/10.6084/m9.figshare.24429058).
Quantitative PCR assay
By the quantitative PCR (qPCR) analysis, the expression of spa gene from 2 of the 6 LFIA-weakly positive isolates showed significantly lower levels than those of the LFIA-positive strain (S. aureus N315, a wild-type strain; see Fig. S3 at https://doi.org/10.6084/m9.figshare.24429058; P = 0.021 and 0.034).
DISCUSSION
S. aureus is a leading cause of bacteremia, infective endocarditis, osteoarticular, skin, and soft tissue, pleuropulmonary, and device-related infections (1). A strong virulence factor called protein A can identify S. aureus in clinical specimens (9). Rapid detection and diagnosis of S. aureus bacteremia enable prompt and appropriate antibiotic therapy.
In 2020, we developed an LFIA assay using a commercial anti-protein A antibody to detect S. aureus in positive blood culture samples which have the sensitivity and specificity of 87.9% and 93.8%, respectively (8). In the present study, we use human immunoglobulin as a conjugate antibody to detect S. aureus in hospitals, which has not yet been reported. This modification has several advantages, including a cost reduction because human immunoglobulin may be prepared in-house from the leftover pool-serum samples. Human immunoglobulin preparation is simple, rapid, and no requirement for laboratory-animal. In addition, the detection limit for LFIA using human immunoglobulin as a conjugate antibody was lower than those of previously developed LFIA using commercial anti-protein A antibody (see Fig. S4 at https://doi.org/10.6084/m9.figshare.24429058).
In this study, neither false-positive nor false-negative results were found when tested with spiked blood culture samples. However, while testing in the laboratories of three hospitals, the LFIA strip failed to detect 3 of the 160 and 7 of 68 samples with colonies and positive blood culture samples, respectively. The genome analysis of one representative of the false-negative isolate revealed a mutation in the spa gene. This mutation can cause a truncated protein A which may affect the protein A expression or cause impaired function of the protein A (unable to bind with human IgG–gold nanoparticles). Brignoli et al. (11) reported a mutation in the spa 5′ UTR sequence affecting the ribosome entry site which is responsible for the loss of protein A expression. In addition, the absence of protein A expression has occurred in geographically distinct strains through several different molecular mechanisms, such as mutation, leading likely to have altered translation, and transcriptional deregulation (11). Therefore, these false-negative results may be due to the low amount or lack of protein A production in some individual strains (12). In addition, spa gene expression was determined among six representatives of weakly positive-LFIA isolates by qPCR. It was found that four isolates had low spa mRNA levels which may correspond to the low amount of protein A. However, the absence of protein A expression may be associated with other factors, such as higher capsule production (11). Brignoli et al. (11) evaluated the expression of a spa in a collection of staphylococcal strains, about 7% of which did not express the spa gene, despite the presence of the gene. Several factors or other changes in the virulence gene expression profile have been reported to influence the spa expression (11, 13). The regulation of spa expression has been found to be complicated which involved multiple factors, including Agr, Rot, ArlR-ArlS, MgrA, SarA, SarS, and SarT (13, 14). It was reported that the upstream promoter sequences were necessary for Agr system regulation of spa expression. The SarS and SarA functioned as the activator and repressor of spa expression, respectively (13). However, the network of the regulation system is complex and still unclear. Therefore, further study should be performed to gain insights into the reasons for the false-negative results of the LFIA for S. aureus detection.
Recently, a silver solution has been reported to enhance the sensitivity of the LFIA test (15–17). We have performed the LFIA test with a silver solution to amplify the signals (see Fig. S5 at DOI: 10.6084/m9.figshare.24429058). However, the reagent was unstable and extremely sensitive to light as suggested by Tsai et al. (9). Moreover, after adding the silver solution, it required an additional 10 min for the final results. Furthermore, there are several factors that affect the signal of LFIA such as the type of buffers and membranes (18). We have investigated the effect of various running buffers, conjugate pads, and nitrocellulose membranes, to select the optimum condition for the best performance of the LFIA strip (8).
For the detection limit of bacterial colonies, the bacterial suspension to a turbidity of 1.0 McFarland standard (~3 × 10^8^ CFU/mL) was serially 10-fold diluted and confirmed by plating on agar for determination of the CFU. However, the McFarland Standard is designed to be used for estimating the concentrations of bacterial cells especially Gram-negative bacteria such as E. coli. This estimate becomes uncertain with organisms outside the normal usage as different species of bacteria differ in size and mass. The numbers are valid only for those microorganisms similar to E. coli (19). The McFarland method has low accuracy for the estimation of the bacterial populations (20). In this study, the limit of the LFIA for detecting S. aureus from bacterial colonies was 10^7^ CFU/mL (10^6^ CFU/reaction). This inoculum could be easily suspended from grown colonies on routine culture plates. In addition, a positive blood culture bottle usually gives a bacterial population of more than 10^7^ CFU/mL. Therefore, the LFIA can be reasonably practical for application in hospitals.
This method has several advantages, including a simple step of sample preparation, extremely easy to use, good performance, rapid, low cost (approximately $2 per test), easy to store, and long shelf life. In addition, special equipment or skilled technicians are not required.
This study provides a preliminary validation of the developed LFIA in three hospitals. Though the number of positive blood culture samples was limited, the results showed that the LFIA can be used to detect S. aureus in hospitals. However, a full performance test should be further evaluated in hospitals with a larger sample number.
In conclusion, the developed LFIA exhibits high sensitivity and specificity for detecting S. aureus in grown blood culture samples. It could be used as an alternative method for rapid identification of S. aureus which contributes to an early diagnosis and facilitates an effective treatment and retards the disease progression. The LFIA may have potential for routine service, particularly in low-resource settings.
MATERIALS AND METHODS
Bacterial strains
A total of 138 bacterial isolates, comprising 79 S. aureus and 59 non-S. aureus, were collected from Hospitals in Thailand between October 2021 and June 2022 (Table 1). All clinical isolates were stored in skimmed milk with 15% glycerol at −20°C and identified by using standard biochemical tests and PCR techniques. S. aureus strain N315 was used as a positive control.
Preparation of human immunoglobulin
Human immunoglobulin was prepared from the pooled serum of healthy volunteers. It was purified according to the instructions of the HiTrap Protein A HP column (Cytiva, Massachusetts, USA; catalog no. 17040201). After purification, the Vivaspin protein concentrator spin columns (20 and 30 kDa MWCO PES; Cytiva, Massachusetts, USA) were used for the concentration of human immunoglobulin in phosphate buffered saline.
Creating and assembling the LFIA
Conjugation of human immunoglobulin antibody and gold nanoparticles
Human immunoglobulin was used to coat the gold nanoparticles. The conjugation process was performed according to the protocol of a previous study (8), except that human immunoglobulin was used as a conjugate antibody with gold nanoparticles (13 nm; Fig. 1). Finally, the labeled conjugate was put onto a conjugation pad using glass fibers (GF33; Whatman Schleicher & Schuell, Dassel, Germany) and dried at 37°C for 2 h, then kept at 4°C for further use.
Preparation of LFIA strips
Chicken anti-protein A polyclonal antibody (1.0 mg/mL; Arista Biological, Allentown, PA, USA; the purity of protein A > 98% at 214 nm by HPLC) and goat anti-human IgG antibody (1.0 mg/mL; Lampire Biological Laboratories, Pipersville, PA, USA) were dispensed to the nitrocellulose membrane (UniSart CN140; Sartorius Stedim Biotech SA) to be the test and the control lines, respectively, by using a lateral flow dispenser (XYZ3000 Dispensing Platform; BioDot Inc., Irvine, CA, USA; 1 µL/cm) and dried at 37°C for 1 h. The four parts of LFIA including sample pad (cytosep 1660; Pall Gelman Sciences), nitrocellulose membrane [UniSart CN140 NCM (Sartorius Stedim Biotech SA)], conjugate pad (GF33; Whatman Schleicher & Schuell), and absorbent pad (Whatman ABS. PAD #470; Whatman Schleicher & Schuell) were assembled as described previously (8). The treated glass fiber conjugate pad, sample pad, and absorbent pad were assembled to the backing card with a 0.2 cm overlap between each component (Fig. 1). Then the LFIA was cut into 4 mm × 6 cm strips using a CM5000 Guillotine Cutter (BioDot Inc., Irvine, CA, USA). The strips were kept at 4°C in a desiccator.
Molecular characterization of S. aureus by spa gene
According to the technique described by Shittu et al. (21), bacterial DNA was extracted using an achromopeptidase enzyme (Sigma-Aldrich, St. Louis, MO, USA). After the 1-min centrifugation, the supernatant was used as a DNA template for the PCR reaction. The protocol and primer for the detection of the spa gene were described previously (22). The forward primer of 5′-(1522) TCAAGCACCAAAAGAGGAAGA (1544)–3′ and the reverse primer of 5′-(1784) GTTTAACGACATGTACTCCGTTG (1806)-3′ were used. PCR reaction contained 200 µM of each deoxynucleotide triphosphate, 1 U Taq polymerase, 1× PCR buffer, 2 mM MgCl_2_, and 0.5 µM of each primer. The final volume was adjusted to 25 µL with sterile water. PCR amplification was performed with the following conditions: initial denaturation step at 94°C for 5 min; 30 cycles of 94°C for 2 min, 60°C for 1 min, and 72°C for 1 min with a final elongation step at 72°C for 7 min and hold at 4°C. PCR products were detected by electrophoresis in 2.0% agarose gel electrophoresis and stained with 0.5 µg/mL of ethidium bromide. A reference strain of S. aureus (NCTC10442) was used as spa gene-positive control.
Detection limit of the LFIA
The concentrations of purified protein A (Arista Biological) that varied from 10^−1^ to 10^−5^ µg/mL were tested with the LFIA strips. The control line and/or test line would appear as a pink-purple line. The presence of both control and test lines indicated a positive result. The presence of only the control line but not the test line indicated a negative result.
To determine the detection limit of the LFIA for bacterial colonies, a 1 µL loop full of bacterial colonies cultured on blood agar (Oxoid, Hampshire, UK) at 35°C for 18 to 24 h was suspended in 1.5 mL microcentrifuge tubes containing 200 µL of distilled water with turbidity of McFarland Standard no. 1.0 (approximately 3 × 10^8^ CFU/mL). Then the bacterial suspension was serially 10-fold diluted from 10^−1^ to 10^−7^, and a bacterial colony count was performed to check the concentration of cells in the suspension. In addition, each bacterial suspension was boiled for 3 min in a heat block at 100°C, and allowed to cool for 2 min, and 100 µL of the 10^0^–10^−5^ dilutions were used as samples. The bacterial solution was dropped into the sample pad of LFIA and added to 100 µL of buffer (Kestrel Bio Sciences, Pathumthani, Thailand). The lowest protein concentration and/or the least colony count that provided a positive result were considered the detection limit.
LFIA imaging and quantitative analysis of signal
The LFIA was imaged with a smartphone (Huawei Nova 2i, Huawei Base, Shenzhen, China) inbuilt camera at a fixed setting (ISO 50). The smartphone camera was placed at a 90° angle and at a distance of 10 cm above the LFIA. The intensity of the test lines was analyzed using ImageJ software (version 1.53a; National Institute of Health, Bethesda, MD, USA). The intensity of the LFIA signal (test line) was expressed as peak area (23).
Detection of S. aureus from spiked blood culture samples
The spiked blood culture samples of 79 and 59 isolates of S. aureus and non-S. aureus, respectively (Table 1), were used to evaluate the efficacy (sensitivity and specificity) of the LFIA strip for direct detection of S. aureus.
The preparation of spiked blood culture samples was performed as described previously (8). Bacterial antigen extraction was accomplished by boiling 1,000 µL of the samples for 3 min in a heat block at 100°C and allowing it to cool for 2 min. Then, 50 µL of the sample was added to 50 µL of buffer (Kestrel Bio Sciences, Pathumthani, Thailand). The total 100 µL of bacterial solution was dropped into the sample pad of LFIA, and the results were read within 15 min with the naked eye (Fig. 3). The results were compared to those of the PCR method, culture, and biochemical tests as the gold standard. In addition, the Staphaurex Plus Latex Agglutination Test (Thermo Scientific., MA, USA) was used to test the isolates with weakly positive and negative results. This test detects both the clumping factor and staphylococcal protein A. Reference strains of S. aureus (NCTC10442) were used as a protein A-positive control.
The LFIA protocol for detection of S. aureus directly from blood culture samples (a) and bacterial colonies (b).
Evaluation of the LFIA for direct detection in bacterial colonies and positive blood culture bottles from hospitals
The results of the sample were classified in a binary manner (Yes/No) as either positive or negative. The performance of the LFIA test for S. aureus detection was blindly evaluated by medical technologists in three hospitals. The LFIA was tested with 221 bacterial colonies and 33 positive blood culture samples in Hospital A. Furthermore, the LFIAs were initially evaluated in 76 and 9 positive blood culture bottles from Hospital B and Hospital C, respectively.
A 1 µL loop full of bacterial colonies cultured overnight on blood agar (Oxoid) at 35°C was suspended in 1.5 mL microcentrifuge tubes containing 100 µL of running buffer (Kestrel Bio Sciences). The suspension was mixed to homogeneity, and boiled for 3 min in a heat block at 100°C, and allowed to cool for 2 min. The suspension was applied to the sample well of an LFIA strip. The result was read within 15 min at room temperature. For the positive blood culture bottles that were flagged by the Microbial Detection System, the samples were tested directly following the protocol for spiked blood cultures, as mentioned above (Fig. 3). The results of the LFIA were compared with the PCR method for spa gene, culture and biochemical tests as the gold standard. In addition, weakly positive- and negative-result strains were subjected to the Staphaurex Plus Latex Agglutination Test for confirmation.
Stability of the LFIA strips
To evaluate the stability of the developed LFIA, the strips were stored under two conditions, at 25°C and 10°C, and tested for their sensitivity and intensity of T-line after the storage at 6, 12, and 24 months.
qPCR assay for spa gene expression analysis
RNA extraction and cDNA synthesis
Six isolates of weakly positive-LFIA representatives were selected for analysis by qPCR, compared with S. aureus N315, a wild-type strain (LFIA-positive). Bacterial colonies of the selected isolates and S. aureus ATCC 25923 strains cultured on blood agar at 37°C for 24 h, were harvested and used for RNA extraction. RNA isolation was performed by the TRIzol method using Trizol reagent (Invitrogen, Waltham, MA, USA) as described by Oo et al. (24). Total RNA concentration was determined using spectrophotometry at 260 nm, and 1 µg total RNA of each sample was subjected to cDNA synthesis using Maxime RT PreMix Kit (iNtRON Biotechnology, Gyeonggi-do, Korea). The total reaction volume was 20 µL per reaction, and the details were generated by following the Maxime RT PreMix Kit protocol. The cDNA was incubated at 45°C for 60 min, followed by RTase inactivation at 95°C for 5 min. cDNA concentration was determined using spectrophotometry at 260 nm, and cDNA was then used for qPCR.
Quantitative real-time PCR
The real-time PCR for spa gene was carried out using 100 ng of cDNA and the primer set as previously described (22). The primers for 16S rRNA (1,478 bp) were as follows: forward, 5′-CCTGGCTCAGGATGAACG-3′and reverse, 5′-AATCATTTGTCCCACCTTCG-3′ (25). The qPCR was performed using SsoAdvanced Universal SYBR Green Supermix (Catalog #1725271, Bio-Rad Laboratories, Hercules, CA) and a real-time PCR instrument (Applied Biosystems QuantStudio 6 Flex Real-Time PCR System). The qPCR conditions were 95°C for 5 min; 40 cycles of 95°C, 15 s; 60°C, 30 s and 72°C, 30 s, respectively. The amplification products were confirmed by a specific melting curve analysis. The relative expression of genes was calculated using the 2^−∆∆Ct^ formula with 16S rRNA as the housekeeping gene, along with S. aureus ATCC 25923 growth control.
Whole-genome sequencing to compare the molecular characteristics of spa gene
We investigated the molecular characteristic of the spa gene from a representative with LFIA false-negative result by whole-genome sequencing. The DNA was extracted by the phenol-chloroform method (26) and submitted to NovogeneAIT Genomics Singapore for WGS. The DNA sequencing was performed on the NovaSeq 6000 system (Illumina, San Diego, CA) generating 150 bp paired-end reads with >30× coverage. The raw reads were assembled de novo and annotated using Unicycler (27) and RAST tool kit (RASTtk) (28) available in the Bacterial and Viral Bioinformatics Resource Center (https://www.bv-brc.org/). Mutations in the spa gene were analyzed by multiple sequence alignment using clustalw2 (https://www.ebi.ac.uk/Tools/msa/clustalw2/) compared with the genome of S. aureus N315, a wild-type strain (LFIA-positive; accession number: BA000018).
Statistical analysis
The expression of the spa gene from qPCR between the S. aureus isolates with LFIA-weakly positive and LFIA-positive was compared using Student’s t-test. The results from the LFIA test and PCR method were compared by using the Z-test for independent proportion (Stata analysis version 10.0, College Station, Texas, USA). The sensitivity, specificity, and 95% confidence interval of the LFIA method were calculated using a free software vassarStats (http://vassarstats.net/) (29) using the PCR method as the gold standard. The difference in triplicate peak area of the LFIA was tested by one-way repeated measures analysis of variance (ANOVA). The differences between the peak areas of each concentration were tested using one-way ANOVA analysis. The P value of ˂0.05 was regarded as statistically significant.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tong SYC, Davis JS, Eichenberger E, Holland TL, Fowler VG Jr. 2015. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev 28:603–661. doi:10.1128/CMR.00134-1426016486 PMC 4451395 · doi ↗ · pubmed ↗
- 2Zhao X, Yuan X, Hu M, Zhang Y, Li L, Zhang Q, Yuan X, Wang W, Liu Y. 2021. Prevalence and characterization of Staphylococcus aureus and methicillin-resistant Staphylococcus aureus isolated from bulk tank milk in Shandong dairy farms. Food Control 125:107836. doi:10.1016/j.foodcont.2020.107836 · doi ↗
- 3Kimmig A, Hagel S, Weis S, Bahrs C, Löffler B, Pletz MW. 2020. Management of Staphylococcus aureus bloodstream infections. Front Med (Lausanne) 7:616524. doi:10.3389/fmed.2020.61652433748151 PMC 7973019 · doi ↗ · pubmed ↗
- 4Karnatovskaia LV, Festic E. 2012. Sepsis: a review for the neurohospitalist. 2012. Neurohospitalist 2:144–153. doi:10.1177/194187441245333823983879 PMC 3726110 · doi ↗ · pubmed ↗
- 5Giuliano C, Patel CR, Kale-Pradhan PB. 2019. A guide to bacterial culture identification and results interpretation. P T 44:192–200.30930604 PMC 6428495 · pubmed ↗
- 6Guidry AJ, Squiggins KE, Vann WF, Westhoff DC. 1991. Prevention of nonspecific binding of immunoglobulin to Staphylococcus aureus protein A in ELISA assays. J Immunol Methods 143:159–165. doi:10.1016/0022-1759(91)90041-d 1940386 · doi ↗ · pubmed ↗
- 7Huang S-H, Wei H-C, Lee Y-C. 2007. One-step Immunochromatographic assay for the detection of Staphylococcus aureus. Food Control 18:893–897. doi:10.1016/j.foodcont.2006.05.005 · doi ↗
- 8Srisrattakarn A, Tippayawat P, Chanawong A, Tavichakorntrakool R, Daduang J, Wonglakorn L, Lulitanond A. 2020. Development of a prototype lateral flow immunoassay for rapid detection of Staphylococcal protein A in positive blood culture samples. Diagnostics (Basel) 10:794. doi:10.3390/diagnostics 1010079433036348 PMC 7601020 · doi ↗ · pubmed ↗