Analysis of Variation in the Origin of the Obturator Artery in Midwestern American Donor Bodies
Corey Diemer, Brynn Schubert, Sara Funk, Shanu Markand

TL;DR
This study examines the variation in the origin of the obturator artery in Midwestern American donor bodies, finding that over half have an abnormal origin, which could impact surgical procedures.
Contribution
The study provides new data on the prevalence of anatomical variations in the obturator artery's origin in a specific Midwestern American donor population.
Findings
54.5% of obturator arteries had an aberrant origin.
16.7% originated from the inferior epigastric artery.
Anatomical variations were found to be common and clinically relevant.
Abstract
The obturator artery (OA) is typically a branch of the anterior division of the internal iliac artery. However, an aberrant obturator artery origin may lead to clinical complications. Because of its location in the pelvic cavity, the OA is at high risk of injury or laceration during a variety of pelvic surgeries. Regarding this, variations in the origins of the OA may result in bleeding that can often be overlooked, rendering treatment ineffective. Our study aimed to assess the origins and course of the OA in Midwestern American donor bodies. Sixty-two donor bodies were obtained from the Gift of Body Donation Program at A.T. Still University’s Kirksville College of Osteopathic Medicine. The origin of each OA was documented and photographed. The OA was identified by observing the vessel's passage through the obturator foramen. Of 132 OAs studied, 72 (54.5%) had an aberrant OA. Further,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
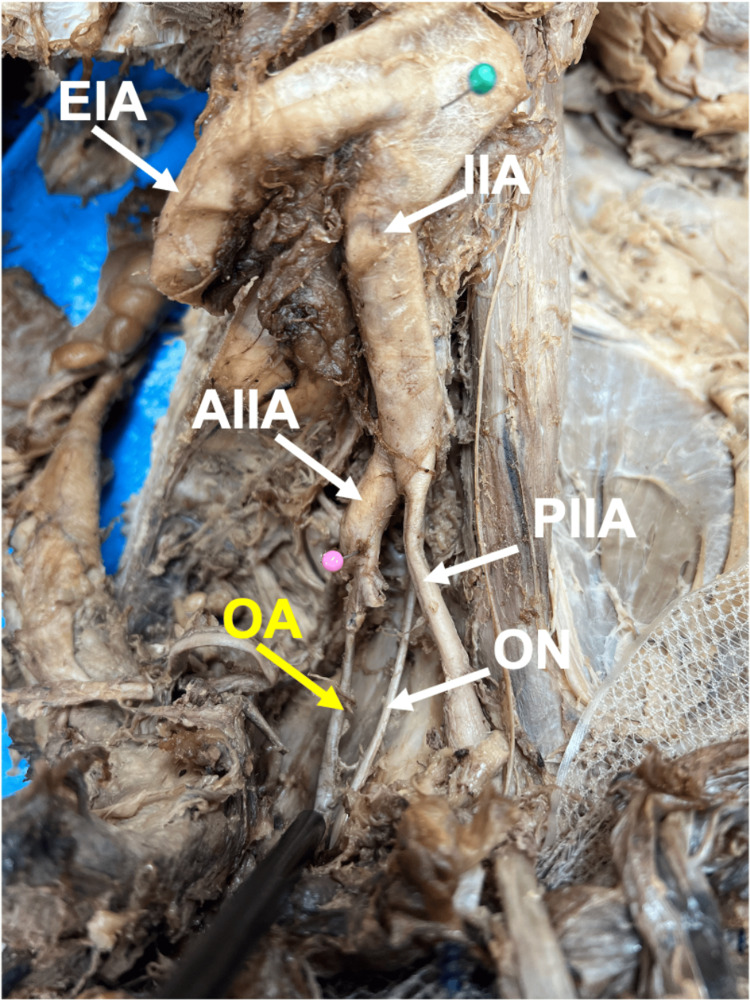 Figure 1
Figure 1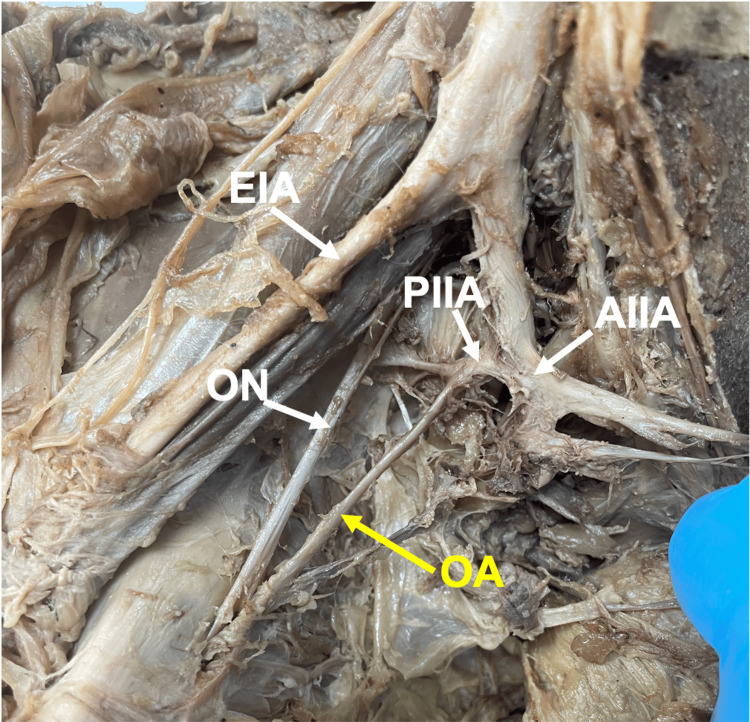 Figure 2
Figure 2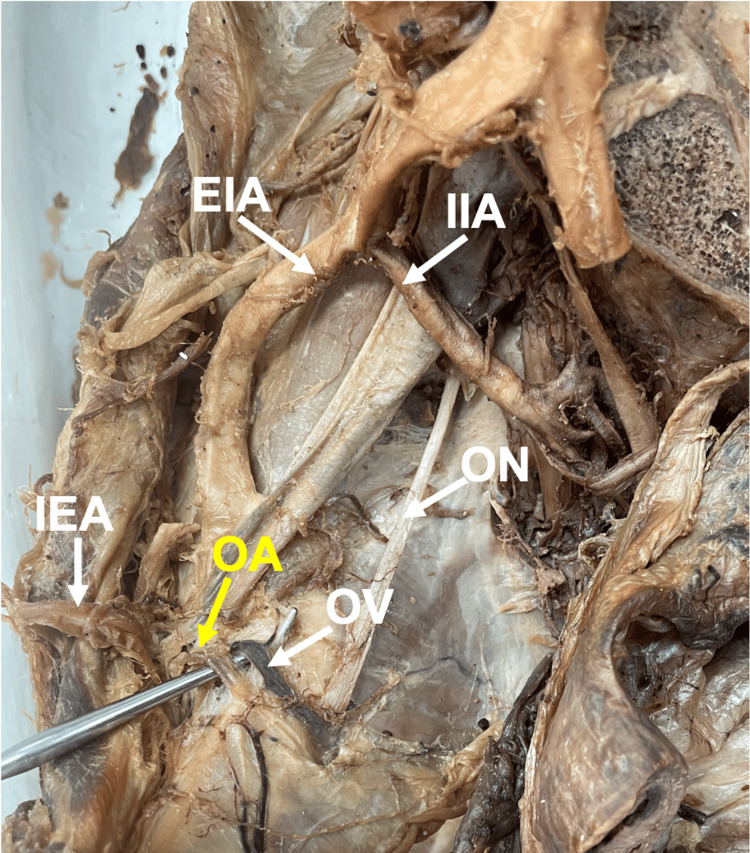 Figure 3
Figure 3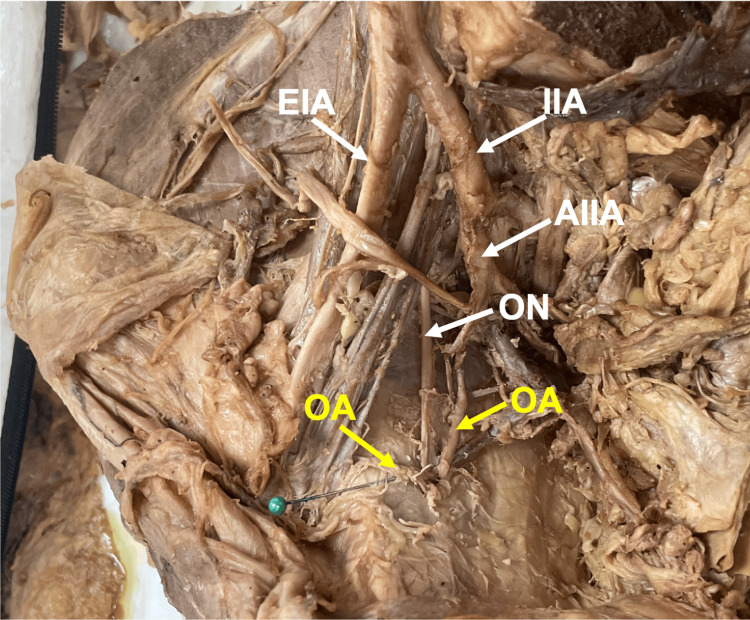 Figure 4
Figure 4| OA Origin | No. (%) Female | No. (%) Male | ||||
| Total (n=77) | Left (n=38) | Right (n=39) | Total (n=55) | Left (n=27) | Right (n=28) | |
| Anterior division of the internal iliac artery | 25 (32.5) | 11 (29.0) | 14 (35.9) | 35 (63.6) | 19 (70.4) | 16 (57.1) |
| Posterior division of the internal iliac artery | 15 (19.5) | 8 (21.1) | 7 (18.0) | 5 (9.1) | 2 (7.2) | 3 (10.7) |
| Inferior epigastric artery | 16 (20.8) | 9 (23.7) | 7 (18.0) | 6 (10.9) | 3 (11.1) | 3 (10.7) |
| Corona Mortis | 16 (20.8) | 8 (21.1) | 8 (20.5) | 6 (10.9) | 2 (7.4) | 4 (14.3) |
| Other | 5 (6.5) | 2 (5.3) | 3 (7.7) | 3 (5.5) | 1 (3.7) | 2 (7.1) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPelvic and Acetabular Injuries · Hernia repair and management · Urological Disorders and Treatments
Introduction
Anatomy of the obturator artery
The obturator artery (OA) is a terminal branch of the abdominal aorta within the pelvic ring. The abdominal aorta bifurcates into the right and left common iliac arteries [1]. Each common iliac artery typically branches into internal and external iliac arteries [1]. External iliac arteries (EIAs) provide the main blood supply to each lower limb [1]. The internal iliac arteries (IIAs) and their branches supply blood to the pelvis, perineum, and gluteal regions [1]. The IIA is further divided into anterior and posterior divisions, with the OA typically originating from the anterior division [1]. The OA travels through the obturator foramen with the obturator nerve and supplies the iliac bone (nutrient branch), obturator externus, iliacus, adductor magnus, adductor minimus, adductor longus, adductor brevis, pectineus, and gracilis muscles [1].
Variation in the obturator artery
Human anatomy studies suggest variations in the origin of the OA are common [1-10]. An aberrant obturator artery (AOA) is a vessel of an atypical origin and location. Specifically, the OA does not originate from the anterior division of the IIA. When AOAs are found, the most common origin is the inferior epigastric artery or the EIA [1,5]. One potentially fatal variation occurs when an anastomosis forms between the OA and the inferior epigastric artery so that the artery courses over the superior pubic ramus [11]. As suggested by its name of corona mortis or “crown of death,” this presentation causes an increased risk of ligation or injury during surgical interventions or pelvic fractures. Previous studies have suggested a lack of awareness and familiarity with AOA are associated with potentially life-threatening outcomes during clinical procedures [2,12]. However, these studies utilized limited donor bodies to investigate AOA. More studies with larger sample sizes are necessary to characterize the occurrence of AOAs across United States demographic groups. Further, there is paucity in the literature regarding the prevalence of AOAs in the Midwestern American population. To address these limitations, our study aimed to assess the origins and course of the OA in Midwestern American donor bodies.
Materials and methods
All procedures in the current study were considered exempt by the A.T. Still University-Kirksville Institutional Review Board. The current study was part of a Gross Anatomy dissection course. It used 62 donor bodies of Midwestern Americans from the Gift of Body program at A.T. Still University’s Kirksville College of Osteopathic Medicine. The average age was 74.71 years old, while the range was 29-98 years old. Exclusion criteria for selecting donor bodies were autopsy, donating major organs, gross obesity, destructive trauma, extensive surgery, and communicable disease. The donor completed a brief medical history, or the next-of-kin donation filled out the medical history at the time of death. Five pelvic halves (one female, four male) were excluded from the study due to extensive trauma from previous pelvic surgery or previous dissection, resulting in the destruction of the OA and associated structures. OAs from 121 pelvic halves (69 female and 52 male) were dissected. The dissections were performed using donor bodies in the spring of 2022 and 2023. Dissections from the spring of 2022 studied 64 total OAs (32 female OAs, 32 male OAs) from 29 female and 30 male pelvic halves. Dissections from the spring of 2023 studied 68 total OAs (45 female OAs, 23 male OAs) from 40 female and 22 male pelvic halves. The initial discovery of the OA was made by Gross Anatomy students. To assess the origins and course of the OA, additional dissection of donor bodies beyond course requirements was performed by the authors specifically to reveal the OA and associated structures. Each donor body's origin and course of each OA were identified as they passed through the obturator foramen and were documented and photographed using an iPhone 12 Pro camera. Frequency and percentage (%) were used to summarize OA variation findings overall by sex and by left and right pelvic halves.
Results
Table 1 summarizes our comparisons of the origins of the OA between female and male donor bodies in the left and right pelvic halves. The prevalence of normal origins of OA anatomy was more prevalent in male donor bodies (left = 70.4%, right = 57.1%). Female donor bodies more often had aberrant anatomy (67.5%), where the OA originated from the IIA posterior division (19.5%), the inferior epigastric artery (20.8%), the corona mortis presentation (20.8%) or other origins (6.5%). In female and male donors, percent (%) were calculated relative to the right or left hemipelvis. Raw data are available in the appendix.
Figure 1 presents the typical origin and course of the OA. Of the 132 OAs dissected during the study, 60 (45.5%) had normal anatomy, where the OA originated from the anterior division of the IIA. Seventy-two (54.5%) of the 132 had AOA origins. Of the 60 (45.5%) normal OA origins, 25 (18.9%) OA origins were from female donors, and 35 (26.5%) OA origins were from male donors. Percents (%) were calculated relative to total OAs in the study.
Typical anatomy of the obturator artery (OA, yellow) originating from the anterior division of the internal iliac artery (AIIA, pink pin). As shown, the OA anatomy typically originates from the anterior division of the IIA; the OA (yellow label) arises from the anterior division of the IIA (pink pin indicates AIIA). The image is from a male donor body, right hemipelvis.Abbreviations: IIA, internal iliac artery; EIA, external iliac artery; ON, obturator nerve; PIIA, posterior division of the IIA
Twenty (15.2%) OAs originated from the posterior division of the IIA (Figure 2). Of the 20 (15.2%) OAs originating from the posterior division of the IIA, 15 (11.4%) OA origins were from female donors, and five (3.8%) OA origins were from male donors. Percents (%) were calculated relative to total OAs in the study.
The obturator artery (OA) originates from the posterior division of the internal iliac artery (PIIA). As shown, the anterior and posterior divisions of the IIA originated from the IIA. Specifically, the OA (yellow label) originates from the posterior division of the IIA. The image is from a female donor body, right hemipelvis.Abbreviations: IIA, internal iliac artery; AIIA, anterior division of IIA; EIA, external iliac artery; ON, obturator nerve
Twenty-two (16.7%) originated from the inferior epigastric artery (Figure 3). Of the 22 (16.7%) OAs originating from the inferior epigastric artery, 16 (12.1%) OA origins were from female donors, and six (4.6%) OA origins were from male donors. Percents (%) were calculated relative to total OAs in the study.
Aberrant obturator artery (OA) originating from the inferior epigastric artery (IEA). The OA (yellow label and a probe) originates from the IEA. As the probe indicates, OA is accompanied by the obturator vein (OV). The image is from a female donor body, right hemipelvis.Abbreviations: IIA, internal iliac artery; EIA, external iliac artery; ON, obturator nerve
Twenty-two (16.7%) OAs originated from the IIA anterior division and inferior epigastric artery (Figure 4), presenting with corona mortis. Of the 22 (16.7%) corona mortis origins, 16 (12.1%) were from female donors, and six (4.6%) were from male donors. Percents (%) were calculated relative to total OAs in the study.
Dual aberrant obturator arteries (OAs) originate from the anterior division of the internal iliac artery (AIIA) and the inferior epigastric artery. Dual OAs (yellow labels) were observed in 11 pelvic halves. The first OA had typical anatomy originating from the anterior division of the IIA. The second OA is marked with a green pin and originated from the inferior epigastric artery. The image is from a female donor body, left hemipelvisAbbreviations: IIA, internal iliac artery; EIA, external iliac artery; ON, obturator nerve.
Eight (6.1%) OAs arose from other origins, including the EIA, the posterior division of the superior gluteal artery, and the inferior vesicle artery. Of the eight (6.1%) other origins, five (3.8%) OA origins were from female donors, and three (2.3%) OA origins were from male donors. Percents (%) were calculated relative to total OAs in the study.
Discussion
Anatomical variations in OA are widespread [1,3,4,6,11,13-15] and may have a major impact on clinical diagnosis, interventions, and patient safety. Therefore, understanding the prevalence of OA variations and their associated complications is necessary to enhance diagnostic studies, preoperative planning, operative decisions, and overall surgical safety, particularly for procedures in the pelvic region. Of our study's 62 Midwestern American donor bodies, we observed aberrant OA origins in 54.5% of pelvic halves.
Previous studies have reported AOA origins with a prevalence of 22%-60% [1,3,4,6,11,13,14]. These findings underscore the likelihood of encountering AOA during operative procedures. For instance, Granite et al. [1] found that 38.9% of cadavers in their study had an anomalous OA origin, and some had bilateral anomalous origins, with 33% originating from the inferior epigastric artery and 5.6% from the EIA. A study by Rajive and Pillay [15] reported additional aberrant origins that were unobserved in our study. Specifically, they found OAs originating from the inferior epigastric artery, from both the IIA and EIA, and the posterior trunk of the IIA, superior gluteal artery, inferior gluteal artery, and pudendal artery [15]. We observed similar variations in our study, especially OA arising from the inferior epigastric and the posterior division of the internal iliac. Studies also support the prevalence of AOA and emphasize sex-specific differences in findings [4,13,15]. In our study, female donor bodies had AOA more often than males bilaterally.
The clinical importance of recognizing vascular variations, particularly about unknown or unidentifiable bleeding during pelvic injuries or procedures, is well documented [1,6,11,15]. In a meta-analysis of studies from 1952-2020, Brachini et al. [16] reported that an average of 22.3% of patients had AOA. In another study, Perandini et al. [11] reported a prevalence of corona mortis due to AOA in 40.6% of 150 patients, highlighting the importance of surgeon awareness and preoperative assessment. We report 16.7% of 132 OA with corona mortis presentation. Notably, corona mortis, which involves an anastomosis between the OA and inferior epigastric artery, increases the risk of surgical complications [17-20]. Therefore, the potential for life-threatening bleeding underscores the importance of identifying OA variations that lead to corona mortis [2,11,15,17,18,20].
As such, some have advocated for preoperative diagnostic tools to enhance patient safety and reduce surgical complications. For example, Brachini et al. [16] recommended radiological examination to determine pelvic vasculature patterns that could contribute to improved patient care. Similarly, Requarth and Miller [4] showed that computed tomography angiography had high sensitivity for identifying AOA origins. Others have measured OA diameters and reported significant variability that ranged from 1.63 mm to 28.3 mm [11,19,20]. In their study investigating different aspects of OA anatomy, Sañudo et al. [14] noted variations in the number of OA origins, where 96.55% of OA had a single origin, 3.02% had a double origin, and 0.43% had a triple origin. These studies, including our own, reflect the importance of exploring AOA findings in ways unique to most OA studies thus far. The more variability in OA origins is understood, the more preparation can be applied to surgical cases.
Strengths of our study include a sample size of 62 donor bodies, high-quality images, inclusion of both sexes, and wider age range (29-98 years old). Limitations of this study include a sample population from a limited geographical location, a lack of other live imaging modalities, and a lack of data on the length and diameter of the OAs as we focused on origins only. Future studies will explore including different imaging modalities to supplement data obtained from donor bodies.
Conclusions
The current study assessed the origins and course of the OA in Midwestern American donor bodies. Fifty-four percent of OAs were aberrant, with the most common variation being an inferior epigastric and posterior division of the internal iliac artery. AOAs were more common in females than males. Our data highlighted anatomical variations in the origin of the OA. These variations may have important surgical implications for interventions of the pelvis, the risk of hemorrhage from pelvic fractures, and overall patient safety. Therefore, surgeon awareness of the prevalence of these variations is critical in preventing or stopping pelvic bleeds during surgery. Further, familiarity with variations in OA origin may have implications for vascular and orthopedic surgeons.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Frequency and clinical review of the aberrant obturator artery: a cadaveric study Diagnostics (Basel) Granite G Meshida K Wind G 10202010.3390/diagnostics 10080546 PMC 745997932751771 · doi ↗ · pubmed ↗
- 2Anatomical variations of corona mortis in the anterior intrapelvic approach: a cadaveric study Mymensingh Med J Sambhav K Nayyar AK Elhence A Gupta R Ghatak S 826834312022 https://pubmed.ncbi.nlm.nih.gov/35780370/35780370 · pubmed ↗
- 3Variability of the obturator vessels Clin Anat Gilroy AM Hermey DC Di Benedetto LM Marks SC Jr Page DW Lei QF 328332101997 https://pubmed.ncbi.nlm.nih.gov/9283731/928373110.1002/(SICI)1098-2353(1997)10:5<328::AID-CA 7>3.0.CO;2-M · doi ↗ · pubmed ↗
- 4Aberrant obturator artery is a common arterial variant that may be a source of unidentified hemorrhage in pelvic fracture patients J Trauma Requarth JA Miller PR 3663727020112130773510.1097/TA.0b 013e 3182050613 · doi ↗ · pubmed ↗
- 5Unconventional obturator artery nutrient branch: image of an anatomical variation Diagnostics (Basel) Bosse BL Palacios VJ Dutcher DW Etter EJ Lim PC Cobine CA Moritz GL 12202210.3390/diagnostics 12082019 PMC 940716336010369 · doi ↗ · pubmed ↗
- 6Study of variations in the origin of obturator artery Indian J Vasc Endovasc Surg Sonje PD Vatsalaswamy P 13113532016
- 7Clinical importance of a star shaped branch of internal iliac artery and unusual branches of an abnormal obturator artery: rare vascular variations J Vasc Bras Nayak SB Guru A Reghunathan D Maloor PA Padavinangadi A Shantakumar SR 1681721520162993058510.1590/1677-5449.000116 PMC 5829714 · doi ↗ · pubmed ↗
- 8Presence of abnormal obturator artery and an abnormal venous plexus at the anterolateral pelvic wall OA Case Rep Nayak SB Shetty SD Shetty P 4932014 https://www.researchgate.net/profile/Satheesha-B-2/publication/280553442_Presence_of_abnormal_obturator_artery_and_an_abnormal_venous_plexus_at_the_anterolateral_pelvic_wall/links/569345 a 408aec 14fa 55db 7d 2/Presence-of-abnormal-obturator-artery-and-an-abnormal-venous-plexus-at-the-anterolateral-pelvic-wall.pdf