Case report of a successful conservative surgical treatment of a giant liposarcoma of the forearm invading the median nerve
Jamal Karbal, Amine Machmachi, Walid Bouziane, Moncef Amahtil, Ousmane Laye Diene, Abdelkrim Daoudi

TL;DR
A rare case of a large liposarcoma in the forearm was successfully removed surgically without recurrence.
Contribution
Reports a successful conservative surgical treatment of a rare liposarcoma invading the median nerve.
Findings
Complete excision of the liposarcoma resulted in good functional recovery.
No recurrence was observed during a 2-year follow-up period.
Surgical treatment with clear resection margins is effective for localized liposarcomas.
Abstract
Liposarcomas (LPS) are the most common malignant tumors among soft tissue sarcomas. We report a rare case of well-differentiated liposarcoma (lipoma-like) located along the anterior compartment of the right forearm, which was successfully treated with complete excision, resulting in good functional recovery without recurrence during a 2-year follow-up. Surgery is the primary treatment for localized forms, involving complete and radical excision with clear resection margins. LPS represents a heterogeneous group of soft tissue sarcomas, with diagnosis primarily relying on histological examination. Their care requires a multidisciplinary approach.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2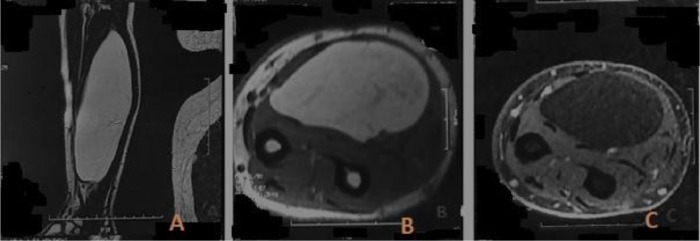 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7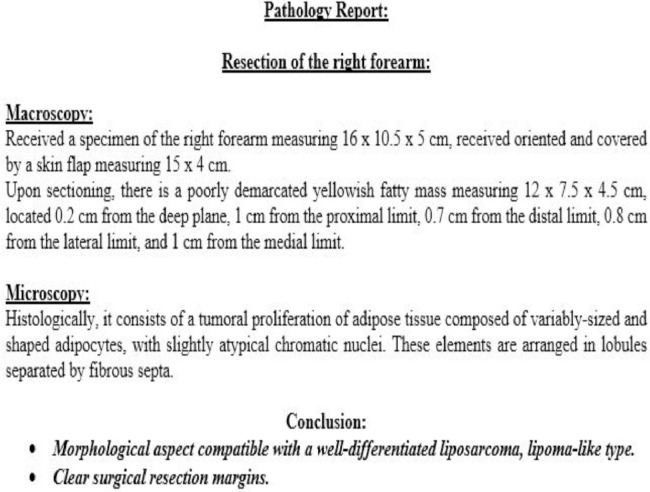 Figure 8
Figure 8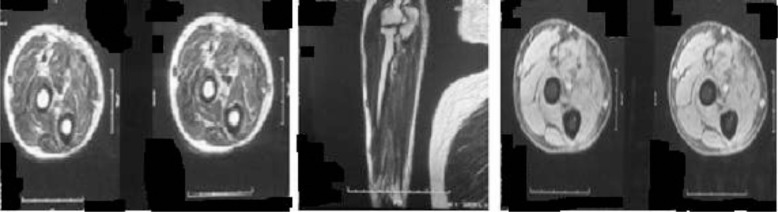 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoma Diagnosis and Treatment · Cardiac tumors and thrombi · Musculoskeletal synovial abnormalities and treatments
Introduction
Liposarcoma (LPS) of the extremities is the second most common soft tissue sarcoma after malignant fibrous histiocytoma, representing 16%-18% of all malignant soft tissue tumors [1], [2], [3], [4], [5]. MRI plays a significant role in diagnosis in the majority of cases due to the presence of fatty components. We present the results of a 48-year-old patient with a large liposarcoma in the anterior compartment of the forearm, in proximity to the median nerve. The patient underwent complete resection, resulting in good functional recovery with no recurrence.
Case report
We report the case of a 48-year-old patient with no significant medical history who presented with an enormous swelling on the right forearm (Fig. 1). This swelling had been present for 1 year and had progressively increased in size to become massive. It caused significant discomfort due to its weight and limited manual activities. The patient also experienced pain and paresthesia radiating into the thenar eminence. Upon clinical examination, the tumor was massive, occupying the entire anterolateral region of the forearm, and measuring 14 cm along its major axis. It was firm to the touch and movable in relation to the deep tissues. There was a decreased sensitivity on the palmar side of the index and thumb, but no motor deficits were observed. The initial radiological assessment, including standard X-rays of the forearm in both anteroposterior and lateral views, revealed no anomalies (Fig. 2). An ultrasound examination showed a well-defined fatty soft tissue mass measuring 86 × 46 mm. To further evaluate the condition, an MRI was performed, revealing a fatty, well-demarcated tumoral process within the anterior compartment of the forearm along the superficial flexors. This mass had close contact with the median nerve, raising suspicion of a lipoma or liposarcoma (Fig. 3).Fig. 1. Giant anterior swelling of the right forearm.Fig 1:Fig. 2. Standard X-ray of the forearm showing no anomalies.Fig 2:Fig. 3. Well-defined homogeneous tumoral process in the anterior compartment of the forearm, subaponeurotic: (A) hyperintense, (B) fat tissue signal, (C) hypointense in contact with the median nerve.Fig 3:
A biopsy was initially conducted, and the results were consistent with a well-differentiated liposarcoma (Fig. 4). Metastatic workup yielded negative results. Subsequently, the chosen therapeutic approach was a conservative surgical procedure, involving en bloc resection of the tumor with a 2 cm safety margin in width and depth. This procedure also required the complete resection of the superficial flexors of the anterior forearm compartment while preserving and meticulously dissecting the median nerve. A tenodesis of the remaining superficial flexors with the deep flexors was performed to maximize finger mobility (Fig. 5, Fig. 6, Fig. 7). The histological examination of the operative specimen confirmed the diagnosis of a well-differentiated liposarcoma of the lipoma-like subtype with clear surgical margins (Fig. 8).Fig. 4. Intraoperative image of the biopsy.Fig 4:Fig. 5. Total tumor resection.Fig 5:Fig. 6. Intraoperative image after complete resection while preserving the median nerve.Fig 6:Fig. 7. View of the tumor specimen.Fig 7:Fig. 8. Histological confirmation results after tumor excision.Fig 8:
The patient had undergone clinical and radiological follow-up with an MRI, which showed the absence of any signs of local recurrence after a 2-year follow-up (Fig. 9). Emphasis was placed on self-rehabilitation of the hand and fingers, leading to a good functional recovery and a return to work after three months.Fig. 9. Follow-up MRI sequences showing no signs indicative of tumor recurrence.Fig 9:
Discussion
Liposarcomas (LPS) are the most common malignant tumors among soft tissue sarcomas and account for approximately 10%-35% of those originating from primitive mesenchymal cells. They typically occur in adults between the ages of 40 and 60, with a higher incidence in males [6]. These tumors are primarily deep-seated, located within or between muscles [[7], [8], [9], [10], [11], [12]]. Clinically, like other soft tissue sarcomas, LPS often manifest as painless soft tissue masses. However, approximately 10%-15% of cases may present with pain [1], [2], [3]. In our case, the mass was located in the superficial finger flexors.
MRI plays a crucial role in investigating LPS, which typically presents as a hypointense signal in T1 and a homogeneous hyperintense signal in T2, with well-defined boundaries, as seen in our case. In addition to its value in assessing local and regional extension (involvement of bone, soft tissues, and vascular-nerve structures), a definitive diagnosis of these tumors can only be made through histological means, requiring a surgical biopsy to be performed before any therapeutic intervention [13].
According to the World Health Organization (WHO), LPS is histologically classified into five groups: well-differentiated, myxoid, pleomorphic, dedifferentiated, and mixed [[1], [2], [3], [4], [5], [6], [7], [8], [9], [10], [11], [12]]. Well-differentiated liposarcoma is the most common histological subtype, accounting for approximately 40%-50% of soft tissue LPS cases [[1], [12], [14], [15]]. Within this type of LPS, five subtypes are distinguished: [16]
- •Well-differentiated adipocytic LPS, also known as lipoma-like, diagnosed by the presence of hyperchromatic atypical cells. This is the histological type of our case, confirmed by the tumor resection specimen.
- •Well-differentiated sclerosing LPS characterized by the presence of fibrous septa that dissect mature adipose tissue, containing atypical cells with pleomorphic and hyperchromatic nuclei.
- •The “inflammatory” variant, characterized by an intratumoral inflammatory infiltrate of polymorphonuclear or lymphoplasmacytic cells, which may raise differential diagnoses with inflammatory or lymphomatous conditions.
- •Well-differentiated spindle cell LPS, a variant described, primarily affecting subcutaneous tissue, especially in the shoulders. It is composed of spindle cells with hyperchromatic, minimally atypical nuclei, often associated with irregular adipocytes and some lipoblasts. This subtype may pose a differential diagnosis challenge with spindle cell lipoma.
- •Dedifferentiated LPS, which always arises from a well-differentiated LPS and is associated with a high-grade nonlipogenic sarcomatous component. This component can resemble malignant fibrous histiocytoma (MFH) with storiform pleomorphic features or fibrosarcoma. Diagnosing this type can be challenging when dealing with biopsies that only involve poorly differentiated areas. Adequate sampling to identify well-differentiated areas is crucial for making this diagnosis.
Surgery remains the primary treatment for localized LPS. Only complete and radical excision with clear resection margins offers a potential curative approach. Postoperative radiotherapy can reduce the risk of recurrence [17]. It is particularly indicated when incomplete resection leaves tumor cells behind to sterilize them. Additionally, it may be considered as palliative treatment for inoperable large tumors. Myxoid LPS is the most radiosensitive subtype. Chemotherapy has limited utility; however, it appears to improve survival rates and reduce the incidence of local recurrences and metastases in larger tumors. In our case, the treatment involved surgical resection of the tumor while preserving the median nerve. The surgery followed ten sessions of radiotherapy to shrink the mass before resection, although the radiotherapy was ineffective in this particular case.
The histological type and grade of the tumor are the primary prognostic factors, and they are correlated with the risk of local recurrences and metastases [18]. Other prognostic factors that have been implicated include the quality of excision, the presence of synchronous metastases, as well as neurovascular and bone involvement [19].
Conclusion
LPS presents challenges in terms of diagnosis and therapeutic management, highlighting the importance of a multidisciplinary, early, and grade-specific decision that aligns with the stage of the condition. This approach enables the possibility of long-term remission.
Patient consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the editor-in-chief of this journal on request.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Peterson JJ Kransdorf MJ Bancroft LWO'Connor MI Malignant fatty tumors: classification, clinical course, imaging appearance and treatment Skeletal Radiol 3220034935031280252010.1007/s 00256-003-0647-8 · doi ↗ · pubmed ↗
- 2Peter LM Lee MJ Janzen D Connell DG Lipoma and liposarcoma: evaluation using CT and MR imaging AJR 1691997589594924278310.2214/ajr.169.2.9242783 · doi ↗ · pubmed ↗
- 3Sung MS Kang HS Lee HG Myxoid liposarcoma: appearance at MR imaging with histologic correlation Radiographics 202000100710191090369010.1148/radiographics.20.4.g 00jl 021007 · doi ↗ · pubmed ↗
- 4Jelinek JS Kransdorf MJ Shmookler BM Aboulatifa AJ Malawer MM.Liposarcoma of the extremities: MR and CT findings in the histologic subtypes Radiology 1861993455459842175010.1148/radiology.186.2.8421750 · doi ↗ · pubmed ↗
- 5SouliéD Boyer B Lescop J Pujol A Le friant G Cordoliani YS.Liposarcome myxoïde J Radiol 761199529367861366 · pubmed ↗
- 6Tewfik JN Greene GS Fluorine-18-deoxyglucose–positron emission tomography imaging with magnetic resonance and computed tomographic correlation in the evaluation of bone and soft-tissue sarcomas: a pictorial essay Curr Probl Diagn Radiol 3720081781881850232510.1067/j.cpradiol.2007.10.005 · doi ↗ · pubmed ↗
- 7Peterson JJ Kransdorf MJ Bancroft LWO’Connor MI Malignant fatty tumors : classification, clinical course, imaging appearance and treatment Skeletal Radiol 3220034935031280252010.1007/s 00256-003-0647-8 · doi ↗ · pubmed ↗
- 8Peter LM Lee MJ Janzen D Connell DG Lipoma and liposarcoma: evaluation using CT and MR imaging AJR 1691997589594924278310.2214/ajr.169.2.9242783 · doi ↗ · pubmed ↗