Pneumocystis jirovecii Pneumonia in a Patient With Localized Mycosis Fungoides Not Receiving Immunosuppressive Treatment
Ryohei Kudoh, Kosaku Komiya, Ryuichiro Takaki, Atsushi Yokoyama, Kazufumi Hiramatsu, Jun-ichi Kadota

TL;DR
A patient with localized mycosis fungoides developed Pneumocystis jirovecii pneumonia without receiving immunosuppressive treatment, highlighting a rare clinical scenario.
Contribution
Reports a rare case of PCP in a patient with localized MF not on immunosuppressive therapy.
Findings
PCP was diagnosed in a patient with localized mycosis fungoides not receiving immunosuppressive treatment.
The patient showed improvement with trimethoprim-sulfamethoxazole, prednisolone, and ganciclovir.
Possible mechanisms for PCP development in this context are discussed.
Abstract
Pneumocystis jirovecii pneumonia (PCP) is the most common opportunistic infection in patients with human immunodeficiency virus (HIV), but it may develop in patients without HIV, whose immune system is suppressed by anticancer or immunosuppressive agents even when indicating normal counts of CD4+ T cells. Mycosis fungoides (MF) is a primary cutaneous T-cell lymphoma, which is believed not to cause immunosuppressive conditions unless it develops leukosis or metastasis or is treated with anticancer drugs or systemic immunosuppressants. Here, we report a case of PCP in a patient with localized MF not receiving immunosuppressive treatment. The patient, a woman in her 70s, presented with persistent dyspnea. High-resolution computed tomography (HRCT) showed diffuse ground-glass opacities in both lungs. Bronchoalveolar lavage fluid was positive for P. jirovecii. Moreover, the cytomegalovirus…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
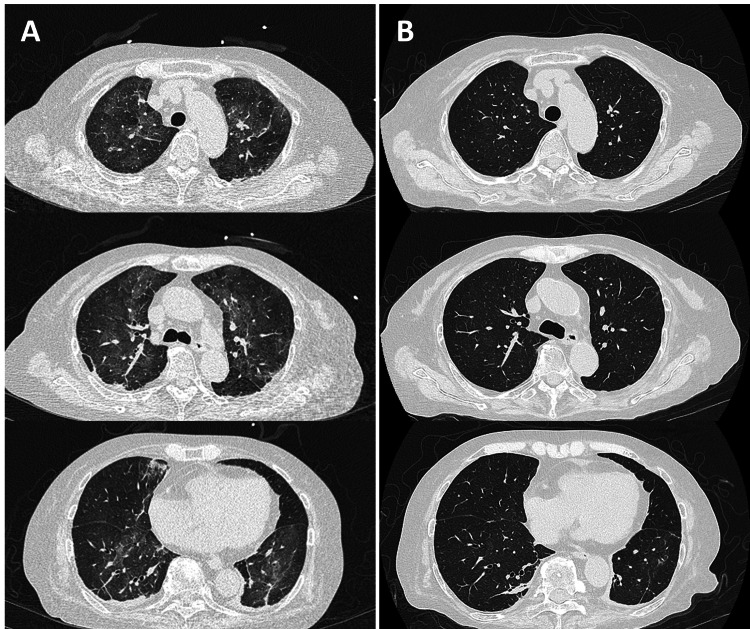 Figure 1
Figure 1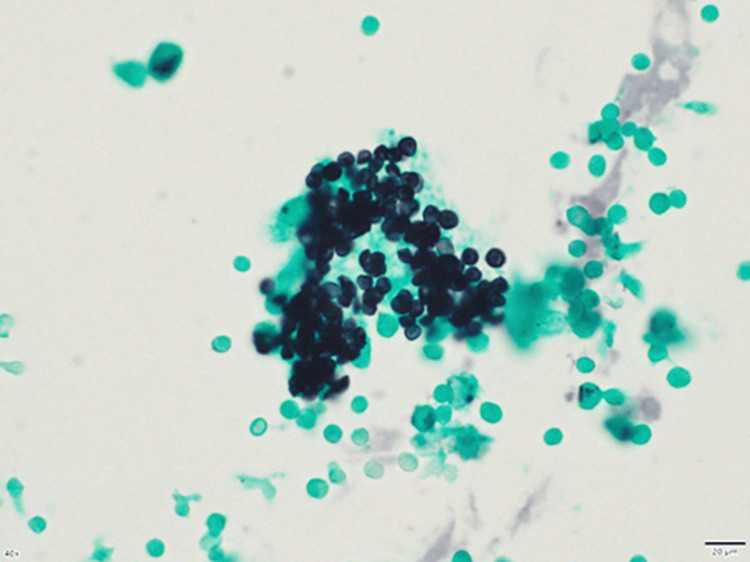 Figure 2
Figure 2| Variables | Result | Reference interval |
| White blood cell, counts/μL | 8,980 | 3,000-7,800 |
| Hemoglobin, g/dL | 13.7 | 10.6-14.4 |
| Serum albumin, g/dL | 2.71 | 4.0-5.2 |
| Blood urea nitrogen, mg/dL | 15 | 7-24 |
| Serum creatinine, mg/dL | 0.33 | <0.7 |
| Lactate dehydrogenase, U/L | 260 | 120-220 |
| C-reactive protein, mg/dL | 6.85 | <0.3 |
| Soluble IL-2 receptor, U/mL | 2,070 | 157-474 |
| D-dimer, μg/mL | 0.47 | <1.0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEosinophilic Disorders and Syndromes · Pneumocystis jirovecii pneumonia detection and treatment · Fungal Infections and Studies
Introduction
*Pneumocystis jirovecii *pneumonia (PCP) is an opportunistic pulmonary infection that affects patients with cell-mediated immunodeficiency, particularly in human immunodeficiency virus (HIV) infection [1]. PCP may also occur in patients with non-HIV immunocompromised status caused by hematologic malignancy, chemotherapy, or immunosuppressants [2]. In recent decades, the prevalence of PCP among non-HIV patients has remarkably increased with more opportunities for receiving chemotherapy or immunosuppressants for postorgan transplantation or autoimmune diseases [3].
Mycosis fungoides (MF) is the most common type of primary cutaneous T-cell lymphoma (CTCL) and is classified as a non-Hodgkin lymphoma [4,5]. MF is clinically characterized by progression from patches to tumors and histologically by an epidermotropic infiltrate of small- to medium-sized CD4+ T cells [6]. Because of primary cutaneous lymphoma, MF is unlikely to suppress the immune system unless it develops leukosis or is treated with anticancer or immunosuppressive agents [7-9]. We encountered a case of PCP that developed in a patient with mild MF without leukosis and prior treatment with anticancer drugs or systemic immunosuppressive agents. To the best of our knowledge, no cases of PCP in a patient with mild MF receiving no systemic immunosuppressive therapy have been reported, whereas atypical pneumonia and opportunistic infections can occur in some immunocompetent individuals. Here, we describe the clinical course and discuss the possible mechanisms of PCP development in our case.
Case presentation
A woman in her 70s was referred to our hospital because of persistent dyspnea for two days. She had been treated for MF with phototherapy and local radiation to the skin of her left lower leg 13 years ago. Etretinate administration and topical steroidal treatment were continued during the visit. She had never received anticancer or immunosuppressive drugs for MF or other diseases. No other history suspicious of noninfectious lung diseases, including hypersensitive pneumonia or drug-induced lung injury, was observed.
Physical examination revealed 36.9°C body temperature, 85% percutaneous oxygen saturation (SpO2) without supplemental oxygenation, 120/62 mmHg blood pressure, and 62 beats/min heart rate. Laboratory blood tests showed increased levels of C-reactive protein, white blood cell count, and soluble IL-2 receptor and decreased serum albumin levels (Table 1). Cytological analysis of peripheral blood did not reveal any atypical cells.
High-resolution computed tomography (HRCT) revealed diffuse ground-glass opacities (GGO) in both lungs (Figure 1A). Polymerase chain reaction (PCR) for severe acute respiratory syndrome coronavirus 2 was negative, but the cytomegalovirus (CMV) antigenemia test (C7-HRP) was positive (46/50000). Beta-D glucan (264 pg/mL) and KL-6 (500.4 U/mL) levels were elevated. Bronchoalveolar lavage fluid (BALF) analysis showed lymphocyte predominance (28.3%), and Grocott’s stain of BALF revealed the presence of *P. jirovecii *(Figure 2), and PCR for P. jirovecii using BALF was positive. Although anti-HIV and antihuman T-cell lymphotropic virus 1 (HTLV-1) antibodies were both negative, the CD4+ T-cell count (281/µL) was moderately low.
Chest high-resolution computed tomography at the patient’s first visit (A) and 13 days after treatment initiation with trimethoprim–sulfamethoxazole, prednisolone, and ganciclovir (B).
Grocott staining reveals capsular dots in the bronchoalveolar lavage fluid, consistent with Pneumocystis jirovecii infection.
The patient was ultimately diagnosed with PCP and CMV infection associated with MF. Treatments with trimethoprim-sulfamethoxazole (720 mg/day as trimethoprim) and prednisolone (40 mg/day) for PCP and ganciclovir (500 mg/day) for CMV infection were initiated. Follow-up HRCT 13 days after treatment initiation (day 13) revealed that the GGOs in both lungs diminished (Figure 1B). The patient’s respiratory status improved to not require oxygen supplementation on day 15, and PCP treatment was completed on day 21. Ganciclovir was administered for 22 days until negative confirmation for the C7HRP antigen. The patient was discharged on day 28 with trimethoprim-sulfamethoxazole continued as the prophylactic dose.
Discussion
The present case was a rare combination of PCP complicated with CMV infection that developed against the background of mild MF with no leukosis or treatment with anticancer or immunosuppressive drugs. Only one case of PCP associated with MF has been reported; however, the patient was treated with systemic glucocorticoids [10]. The possible reasons for the unexpected presentation in the current case need to be discussed.
Several systemic immunodeficiency mechanisms in patients with CTCL are considered. One hypothesis states that antagonization against antitumor immunity induces an immunosuppressive condition. For example, the Jak3/Stat3 pathway is activated in malignant CTCL cells, leading to the production of IL-10 and TGF-β [11-13]. Both cytokines may suppress both cellular and antitumor immunity. IL-10 attacks macrophages, weakens their antigen-presenting ability, and directly suppresses CD4+ T-cell activation [14]. TGF-β inhibits Th1 and Th2 cell differentiation and induces Treg differentiation [15]. The cell surfaces of malignant T cells also express PD-1, PD-L1, and CTLA-4, which act as immunosuppressive proteins [16,17]. PD-L1 binding to PD-1 suppresses T-cell proliferation and production of injurious factors [18]. Furthermore, CTLA-4 binds to CD80 and CD86, competing with CD28 and consequently suppressing T-cell activation [19]. Although clinical evidence of the abovementioned biomarkers is limited, and we did not measure these cytokines in the current case, CTCL may have suppressed the immune system through the mechanisms described, even in mild MF. In fact, the patient’s CD4+ T-cell counts (281/µL) were found moderately low, presumably because of IL-10 production associated with anticancer immunity. The prophylactic administration of trimethoprim-sulfamethoxazole is recommended for patients with HIV having low CD4+ T-cell counts (< 200/µL) or those with PCP history regardless of the CD4+ T-cell counts. While no solid indication for non-HIV patients has been established, our case continued trimethoprim-sulfamethoxazole as the prophylactic dose after the treatment.
In some cases of PCP associated with CTCL other than MF, atypical cells were all found in the peripheral blood, and the condition was diagnosed as leukosis [7,8]. No atypical cells were found in the peripheral blood in the present case; however, the smear test was performed only once. Leukosis complicated with MF is known as Sezary syndrome [4], and repeated blood smear tests or bone marrow biopsy may be required. Similarly, HTLV-1 infection is a known risk for opportunistic infection, but the antibody test was negative in the current case.
Conclusions
Patients with mild MF who did not receive anticancer or immunosuppressive agents may be susceptible to opportunistic diseases, such as *P. jirovecii *pneumonia or CMV infection. Pneumonia that develops in patients with CTCL needs to be differentiated from those caused by atypical pathogens in addition to noninfectious lung diseases. Measuring cytokines and other markers is advisable to confirm immunosuppression. Furthermore, repeated peripheral blood cytology tests or bone marrow biopsy may be required to monitor leukosis or Sezary syndrome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pneumocystis pneumonia N Engl J Med Thomas CF Jr Limper AH 2487249835020041519014110.1056/NEJ Mra 032588 · doi ↗ · pubmed ↗
- 2Clinical, diagnostic, and treatment disparities between HIV-Infected and non-HIV-infected immunocompromised patients with pneumocystis jirovecii pneumonia Respiration Salzer HJ Schäfer G Hoenigl M 52659620182963525110.1159/000487713 · doi ↗ · pubmed ↗
- 3Increasing pneumocystis pneumonia, England, UK, 2000-2010 Emerg Infect Dis Maini R Henderson KL Sheridan EA Lamagni T Nichols G Delpech V Phin N 3863921920132362234510.3201/eid 1903.121151 PMC 3647665 · doi ↗ · pubmed ↗
- 4Mycosis fungoides and Sézary syndrome: an update Hematol Oncol Clin North Am Larocca C Kupper T 1031203320193049766810.1016/j.hoc.2018.09.001PMC 7147244 · doi ↗ · pubmed ↗
- 5Cutaneous lymphoma incidence patterns in the United States: a population-based study of 3884 cases Blood Bradford PT Devesa SS Anderson WF Toro JR 5064507311320091927933110.1182/blood-2008-10-184168 PMC 2686177 · doi ↗ · pubmed ↗
- 6Primary cutaneous T-cell lymphomas other than mycosis fungoides and Sézary syndrome. Part I: clinical and histologic features and diagnosis J Am Acad Dermatol Stoll JR Willner J Oh Y 107310908520213394009810.1016/j.jaad.2021.04.080 · doi ↗ · pubmed ↗
- 7Smoldering adult T-cell leukemia complicated with pneumocystis pneumonia: a case report Respir Med Case Rep Kawamoto K Yamasaki M Taniwaki M 1014043320213440125510.1016/j.rmcr.2021.101404 PMC 8348172 · doi ↗ · pubmed ↗
- 8Adult T-cell leukemia/lymphoma complicated by Pneumocystis pneumonia in a non-endemic area Respir Med Case Rep Kunimoto M Inomata M Chin H 1018074220233666006910.1016/j.rmcr.2023.101807 PMC 9843483 · doi ↗ · pubmed ↗