Assessment of osteoporosis knowledge and its determinants among tuberculosis patients in tertiary care hospital Malaysia: A prospective study
Zohra Bhatti, Madeeha Laghari, Amer Hayat Khan, Bandeh Ali Talpur, Syed Azhar Syed Sulaiman

TL;DR
This study found that most tuberculosis patients in Malaysia have poor knowledge about osteoporosis, with factors like gender, income, and education affecting their understanding.
Contribution
The study identifies key demographic factors influencing osteoporosis knowledge among TB patients in a Malaysian hospital setting.
Findings
61.72% of TB patients had poor osteoporosis knowledge.
Male gender, low income, rural residence, and low education levels were significantly associated with poor knowledge.
The average OKT score was 10.5 out of a possible higher score, indicating limited understanding.
Abstract
Osteoporosis self-care knowledge is essential to encourage the patient’s contribution towards controlling the disease. Osteoporosis incidence with various infectious diseases prompts us to conduct a study on osteoporosis knowledge among Tuberculosis (TB) patients. This study aimed to assess osteoporosis-related knowledge and its influencing factors among TB patients. A prospective cross-sectional study was conducted in the TB clinic of Hospital Pulau Pinang, Malaysia, and an osteoporosis knowledge test (OKT), a structured questionnaire, was used to collect data. TB patients aged 18 years and above with compromised bone health were included in the present study. Overall knowledge scores were dichotomized, calculating the mean score, descriptive statistics, and multivariate regression analysis was used to determine the influence of risk factors on knowledge scores. Of 337 patients,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
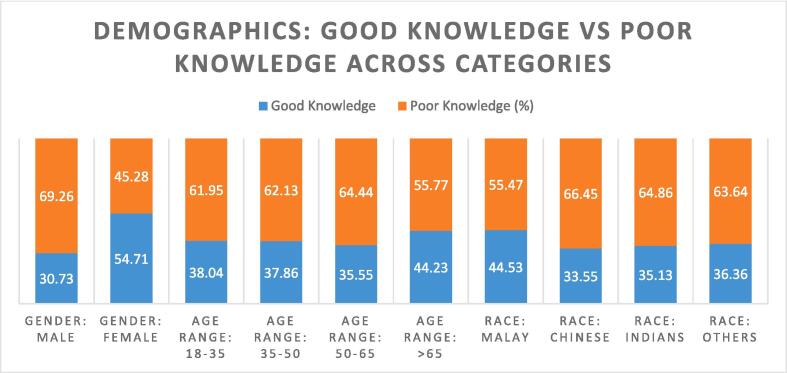 Figure 1
Figure 1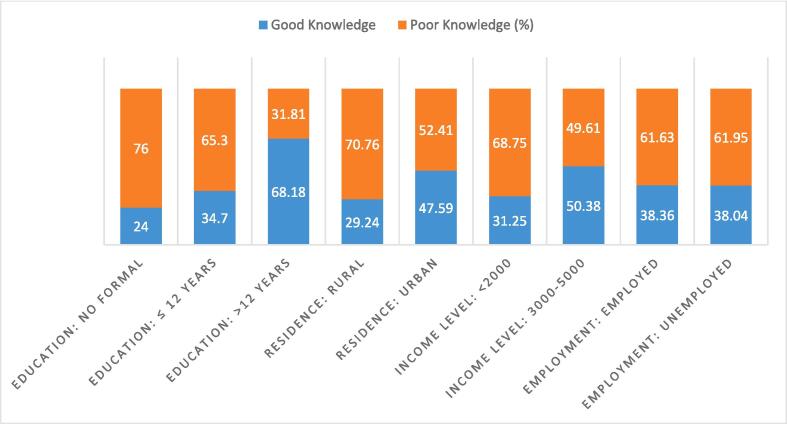 Figure 2
Figure 2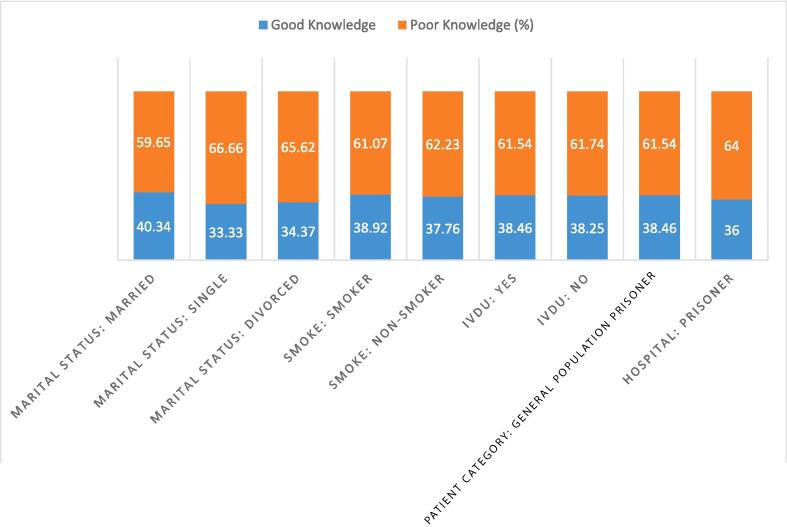 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone health and osteoporosis research · Hematological disorders and diagnostics · Biomarkers in Disease Mechanisms
Introduction
1
Osteoporosis, a disease characterized by reducing bone mass and weakening of bone microstructure, compromised bone strength, and intensifying the risk of fracture, is a growing health hazard around the world. The prevalence of osteoporosis was 10.6 % among the Malaysian male population [1]. Another study revealed that 15.3 % of Malaysian Chinese aged ≥40 years and 32.6 % of those aged 71 years had osteoporosis [2]. Approximately 90 per 100,000 hip fracture incidence rate was reported annually in Malaysia [3].
A study conducted in a university hospital in Zürich has reported association of respiratory TB with bone fracture, even without comorbidities or steroid use, bone degrading was reported in 3––5 % of active TB cases [4]. In a retrospective study conducted in Taiwan, the risk of osteoporosis was presented as 1.36-folds higher among respiratory TB as compared to non-respiratory TB patients. The overall incidence of osteoporosis was 9.61 per 1000 person-years among respiratory TB, as reported by the National Health Insurance Research Database of Taiwan [5]^.^ The osteoporosis incidence rate was 2.2 % among the TB patients and 1.1 % in non-TB patients. Similarly, female TB patients were more likely at risk of osteoporosis than male TB patients [6]. Another retrospective study conducted in Korea reported a 58.6 % prevalence of osteopenia and 14.6 % of osteoporosis among TB patients [7].
The prevalence rate of above-mentioned comorbid conditions reveals TB patients at high risk of osteoporosis. This comorbid condition urges us to attempt a survey to know about the knowledge level of this disease among TB patients. Various osteoporosis studies primarily focus on female gender, pre- and postmenopausal conditions, and adults in different communities. Osteoporosis knowledge assessment studies have been conducted with diverse comorbid conditions like cancer [8], thalassemia [9], HIV [10], and diabetes [11], [12]. The data on osteoporosis knowledge assessment among TB patients is scarce. However, to our knowledge, the current study is the first to evaluate the level of osteoporosis awareness among TB population. Knowledge assessment of osteoporosis disease is vital for controlling and improving patients' health outcomes. Osteoporosis knowledge assessment was found to be correlated with age, education, and income [13]. An Iranian study indicated that higher education is significantly associated with better knowledge [14]. Similarly, an average knowledge about associated demographic risk factors, smoking, extra coffee intake, physical activity, education and living conditions was reported in Lublin, Poland [15].
Knowledge of potential health complications is a prerequisite for engaging in health-promoting practices. More particularly related to low bone density is the knowledge of dietary, exercise and lifestyle characteristics that contribute to development of osteoporosis. The investigation about osteoporosis among TB patients can offer a unique and ground-breaking facts that enhance our understanding on the association of TB disease and osteoporosis. This study has ability to shed light on the interplay between two diseases and linked implications for patient care and public health. Moreover, the present study contributes to a more holistic approach to patient care by identifying the comprehensive care and better patient outcomes. The insights obtain from this study can provide the base for developing preventive strategies and guidance on lifestyle changes like nutrition and exercise.
The current study aimed to access the knowledge of osteoporosis among TB patients by using OKT, an internationally validated scale, to design better policies for improving osteoporosis awareness and preventive health measurements among TB patients in Malaysia. However, to achieve this goal, it is necessary to first examine and comprehend the basic awareness of TB patients towards osteoporosis. The findings can direct the development of future interventions and educational material to encourage strategies that can potentially slow down and control the osteoporotic complications and improve TB patients' quality of life.
Methods
2
Study settings and population
2.1
This was a descriptive cross-sectional study conducted in the respiratory clinic of Hospital Pulau Pinang; a public sector tertiary care hospital that covers a large proportion of the Pinang population in Northern Malaysia. In this study, the population was comprised of patients diagnosed with drug-susceptible PTB aged ≥18 years who were taking their treatment for more than 30 days. After bone screening, they were also diagnosed with the compromised bone health condition (osteopenia means T-score lies between 1 to −2.4 and osteoporosis means T-score is >−2.5). Around 90 % patients were having osteopenia and 10 % were osteoporotic. These were not taking any medication to treat this condition. Those patients who could communicate, understand the questions, and provide oral informed consent, were eligible for inclusion. However, patients with drug-resistant TB and physical and/or cognitive impairment were excluded from the study because of the complexities of managing drug-resistant TB cases and the need for specialized care.
Sample size and sampling technique
2.2
The required sample size was calculated using the Cochrane formula. Based on the assumption of a 95 % confidence interval, a 5 % margin of error, and a 10 % non-respondent rate, the total calculated sample was 430. Of 430 randomly selected patients, 337 (78.5) accepted to participate in the study. Of those who refused to participate, 39(41.93 %) reported that they had no time to participate, 31(33.33 %) had a lack of interest, whilst 23(24.73 %) did not explain. The questionnaires were distributed in the waiting room for about 20–30 min.
Development of data collection tool
2.3
In the present study, the data was collected using tOKT revised version 2012, which was used with the permission of the developer [16]. The socio-demographic factors including gender, age, education, smoking habit, residence, income level, marital status, employment status, hospital visitors, were collected by self-designed questionnaire. Numerous osteoporosis knowledge studies have utilized the OKT 2012 version (used in the current study) and have shown acceptable reliability and validity. Notably, Malay translated was used and validated in type II diabetic patients in the same settings in Malaysia [11]. Thus, this tool was culturally appropriate and understood by the study participants. The data tool was basically in English and translated into Malaysian by linguistic experts, with forwarding and backward translation. It was pre-tested among 10 physicians and 10 nurses in the respiratory clinic, 10 medical academia experts and updated as required. All domains of scales displayed good internal consistency. The reliability coefficients of the OKT tool (Malay version) were 0.8, which was well within the acceptable limits (Cronbach’s α > 0.7). During the pre-test, the questionnaire was evaluated for its clarity, accuracy, reliability, sensitivity of the subject matter, and cultural acceptability in the region. Before distributing the questionnaire, the oral consent for participating in this study was taken from each patient.
Scoring
2.4
The OKT comprises 32 multiple choice instruments comprising two Knowledge domains: nutrition and exercise. It was designed to measure knowledge of osteoporosis and prevention strategies related to exercise and calcium intake. The two subscales had 14 items in common. The total score for the OKT scale ranges from 0 to 32. The range for the nutrition subscale was from 0 to 26, while that for exercise went from 0 to 20. Responses were recorded as correct or incorrect to calculate the good and poor knowledge scores. If respondents indicated more than one option for a question or if a question remained unanswered, the question was defined as incorrect. In scoring, the question was given one mark for the correct answer, while each inaccurate or unknown answer was marked as 0. The overall knowledge score was obtained by summing up these responses. The patients' knowledge was classified into high and low groups using a cut-off point of 14, based on the previous validation study of OKT- Malay version [11]. Consequently, those with a total score equal to or below the mean were classified as having poor knowledge, whereas those above the mean were considered to have good knowledge.
Statistical analysis
2.5
For statistical data analysis SPSS 24 was used in the present study. Before data entry, manual data cleaning checks were used to identify unreadable marks on questionnaires, blank questions, and wrong coding. After completing the manual check process, frequencies were presented for each response and evaluated for missing answers. Descriptive statistics using frequency distribution tables were used to summarize socio-demographic characteristics and to compute total knowledge scores. Multiple regression analysis was done to study the association between poor knowledge level and demographic factors.
Results
3
Demographic and clinical characteristics of the participants
3.1
The socio-demography of patients is given in Table 1. Of 337 patients, 231(68.54 %) were males, and 106(31.45 %) were females, with a mean age of 46.5 ± 17.1 years. The majority of participants (56.67 %) were living in rural areas. Most of them (69.14 %) reported being currently married. For the level of education, 268(79.52 %) had ≤12 years of education. The proportion of employment was high (72.70 %), but majority of participants (61.72 %) had low monthly income (<2000 RM).Table 1. Demographical characteristics of study participants.CharacteristicsPatients n = 337(%)Gender Male231(68.54) Female106(31.45)Mean age ± S.D (years)46.5 ± 17.10Age range**(years)** 18–3592(27.29) 36–50103(30.56) 51–6590(26.71) >6552(15.43)Race Malays137(40.65) Chinese152(45.10) Indians37(10.97) Others11(3.26)Education No formal education25(7.41) ≤12 years268(79.52) >12 years44(13.05)Smoking Yes188(55.78) No149(44.21)IVDUYes39(11.57)No298(88.43)Residence Rural191(56.67) Urban146(43.32)Income Level <2000208(61.72) 3000–5000129(38.28)Marital Status Single72(21.36) Married233(69.14) Divorce32(9.49)Employment Status No92(27.29) Yes245(72.70)Patient Category General population312(92.58) Prisoners25(7.42)
Analysis of OKT scores
3.2
Most of the study participants had poor scores in the OKT subscale about osteoporosis knowledge (Table 2). 24(7.12 %) of patients correctly answered, “Eating a diet low in dairy products causes high chances of osteoporosis”. For the question, “Parents/grandparent’s osteoporosis makes them more prone to get osteoporosis”, 114(33.83 %) of participants checked the “more likely”, 66(19.58 %) chose “less likely”, 85(25.22 %) indicated “Neutral response”. 116(34.42 %) correctly responded to the statement, “Being a White or Asian woman increases the chance of getting osteoporosis”. 77(22.84 %) respondents correctly answered for, “Smoking daily can cause osteoporosis”. About 215(63.79 %) participants chose “Walking briskly”; 248 (73.59 %) considered “jogging or running as a helpful exercise for reduction of osteoporosis”. Only 125(37.09 %) respondents knew “Broccoli as the best source of calcium”, and 81(24.03 %) accurately chose “Canned sardines as the best source of calcium”. Most participants had poor knowledge regarding the nutrition subscale (Table 2).Table 2. Detail description of OKT questions with frequencies and percentage of correct and incorrect responses.VariablesPercentagesn (%)Risk factors of osteoporosis:Do the following make it more or less likely that someone will develop osteoporosisEating a diet LOW in DAIRY products can cause osteoporosisMore likely24(7.12)Less likely191(56.67)Neutral95(28.19)Don’t know27(8.01)Being menopausal change of lifeMore likely106(31.45)Less likely107(31.75)Neutral91(27.00)Don’t know33(9.79)Having a parent or grandparent who has osteoporosisMore likely114(33.83)Less likely66(19.58)Neutral85(25.22)Don’t know72(21.36)Being a white or Asian womanMore likely116(34.42)Less likely64(18.99)Neutral115(34.12)Don’t know42(12.46)Being elderly ManMore likely199(59.05)Less likely55(16.32)Neutral41(12.16)Don’t know42(12.46)Having ovaries surgically removedMore likely79(23.44)Less likely83(24.62)Neutral114(33.8)Don’t know61(18.10)Taking cortisone (steroids) for a long timeMore likely104(30.86)Less likely70(20.77)Neutral114(33.82)Don’t know49(14.54)Being overweightMore likely140(41.5)Less likely90(26.70)Neutral51(15.13)Don’t know56(16.61)Having an eating disorderMore likely103(30.56)Less likely78(23.14)Neutral84(24.92)Don’t know72(21.36)Consuming more than two alcoholic drinks per dayMore likely91(27.00)Less likely122(36.20)Neutral91(27.00)Don’t know33(9.79)Smoking dailyMore likely77(22.84)Less likely103(30.56)Neutral85(25.22)Don’t know72(21.36)To strengthen bones, it is recommended that a person exercise at a moderately intense level for 30 min a day at least3 days a week33(9.79)4 days a week55(16.32)5 days a week200(59.34)Don’t know49(14.54)Exercise makes bones strong, but it must be hard enough to make breathingJust a little faster83(24.62)Much fast, but talking is possible50(14.84)So fast talking is not possible100(29.67)Don’t know104(30.86)Which Activity is the best way to reduce osteoporosisSwimming82(24.33)Walking briskly215(63.79)Stretching14(4.154)Don’t know26(7.72)Which Activity is the best way to reduce osteoporosisBicycling122(36.20)Yoga87(25.82)Lifting weights51(15.13)Don’t know77(22.84)Which Activity is the best way to reduce osteoporosisJogging or running for exercise248(73.59)Golfing using golf craft14(4.15)Gardening30(8.90)Don’t know45(13.35)Which Activity is the best way to reduce osteoporosisBowling42(12.46)Doing laundry17(5.04)Aerobic dancing165(48.96)Don’t know113(33.53)Which one of the following is the best source of calciumApple45(13.35)Cheese201(59.64)Cucumber13(3.85)Don’t know78(23.15)Which one of the following is the best source of calciumPeanut butter54(16.02)Turkey76(22.55)Canned sardines81(24.03)Don’t know126(37.38)Which one of the following is the best source of calciumChicken68(20.17)Broccoli125(37.09)Grapes35(10.38)Don’t know109(32.34)Which one of the following is the best source of calciumYogurt205(60.83)Strawberries20(5.93)Cabbage29(8.60)Don’t know83(24.63)Which one of the following is the best source of calciumIce cream58(17.21)Grapefruit112(33.23)Radishes56(16.62)Don’t know111(32.93)What is the recommended calcium intake for an adult600 mg to 800 mg daily45(13.35)1000 to 1200 mg daily71(21.07)1400 mg to 1600 mg36(10.68)Don’t know185(54.89)How many glasses of milk an adult should take per day1 glass daily12(3.56)2 glass daily152(45.10)3 or more glasses daily93(27.59)Don’t know80(23.74)What is the best reason for taking a calcium supplementIf a person skips breakfast23(6.83)If a person does not get enough calcium164(48.66)If a person is over 45 years old61(18.10)Don’t know89(26.41)Which vitamin is required for the absorption of calciumVitamin A35(10.38)Vitamin C199(59.05)Vitamin D55(16.32)Don’t know48(14.24)Which is the best source of the vitamin required for the absorption of calciumCarrot46(13.65)Oranges38(11.28)Sunlight113(33.53)Don’t know140(41.54)Which is the best source of the vitamin required for the absorption of calciumSpinach71(21.06)Cheese137(40.65)Salmon52(15.43)Don’t know77(22.85)Which of the following is the recommended amount of the vitamin required for the absorption of calcium for an adult, 50 years old and older****800–1000 IU daily63(18.69)1200–1400 IU daily56(16.62)1600–1800 IU daily55(16.32)Don’t know163(48.36)When is the best time to build strong bonesChildhood51(15.13)Adolescence73(21.66)Young adulthood71(21.06)Don’t know142(42.14)Osteoporosis can be diagnosed byBlood test102(30.27)DXA scan52(15.43)Symptoms85(25.22)Don’t know98(29.08)**Once you have osteoporosis,**There is nothing you can do76(22.55)You can take medication to treat it180(53.41)You must be careful lifting objects49(14.54)Don’t know32(9.49)Correct answers were given in bold and italic.
Of the study participants, 129(38.23 %) patients had good, and 208(61.72 %) had poor OKT knowledge. The mean ± SD of OKT total score was 10.5 ± 2.0. The mean ± SD of the exercise knowledge score was 5.3 ± 3.4, while that of the nutrition knowledge score was 5.0 ± 3.2.
Fig. 1, Fig. 2, Fig. 3 depicted the percentage of knowledge score of study participants against socio-dedemographic characteristics.. Around 54.71 % females and 30.73 % males had good knowledge about osteoporosis. The 66.0 % TB patients who lies in the age range more than >65 years had high score of knowledge. Malaysian population had good knowledge than other races (Fig. 1).Fig. 1. Scores of osteoporosis knowledge scale examined by demographic characteristics.Fig. 2. Socio-economic factors: good knowledge vs poor knowledge across category.Fig. 3. Marital status, Habits and other: good knowledge Vs poor knowledge across categories.
Study participants with highest education (68.2 %) and those having high income (50.38 %) had better awareness compared to other groups (Fig. 2).
In Table 3, multiple regression analysis was performed to assess the influencing factors of poor OKT scores. Male gender (OR 3.86, 95 % CI 1.98–7.53), low-income level (OR 1.92, 95 % CI 1.12–3.30), rural residents (OR 2.49, 95 % CI 1.46–4.27) and participants with no formal education (OR 4.34, 95 % CI 1.11–16.84) or ≤12 years of education (OR 3.63, 95 % CI 1.52–8.65) were significantly responsible for poor OKT score.Table 3. Multiple regression analysis of responsible factors of osteoporosis knowledge scores with demographic characteristics.CharacteristicsβS.EOR (95 % CI)P-valueGender Male1.350.343.86(1.98–7.53)<0.001 Female−1.350.340.25(0.13–0.50)Age range**(years)** 18–350.820.522.27(0.81–6.35)0.11 35–500.480.441.63(0.67–3.91)0.27 50–650.200.441.22(0.51–2.95)0.64 >65−0.590.420.55(0.24–1.26)0.16Race Malays−1.290.910.27(0.04–1.64)0.15 Chinese−1.140.930.31(0.05–1.98)0.22 Indians−1.910.980.14(0.02–1.01)0.05 Others1.310.913.70(0.62–22.09)0.15Education no formal1.460.694.34(1.11–16.84)0.03 ≤12 years1.280.443.63(1.52–8.65)0.04 >12 years−1.460.680.23(0.06–0.88)0.03Income level Low0.650.261.92(1.12–3.30)0.01 High−0.650.260.52(0.30–0.89)Residence Rural0.910.272.49(1.46–4.27)0.01 Urban−0.910.270.40(0.23–6.83) Smoke Yes−0.520.290.59(0.32–1.05)0.07 No0.520.291.69(0.94–3.03)IVDU Yes−0.100.431.10(0.46–2.62)0.81 No−0.100.430.90(0.38–2.13)Patient Category General population−0.140.490.86(0.32–2.29)0.77 Prisoners0.140.491.15(0.43–3.07)
Discussion
4
This study was conducted to assess osteoporosis knowledge among TB patients in Malaysia. According to significant study findings, 61.72 % of TB patients had a lack of osteoporosis knowledge. In line with the current study the knowledge about the source of calcium was reported 50 % [17]. Similarly, several studies consistent with current research reported low exercise knowledge [18], [19]. In another study, the majority of participants incorrectly answered the questions on the OKT scale. The mean OKT score indicated poor osteoporosis-related knowledge [12].
The current study differs from previously conducted studies in certain aspects. First, the present study was conducted among TB patients to evaluate their osteoporosis-related knowledge. Secondly, a scoring system was developed for OKT, and participants' scores for each domain were analyzed and correlated with various socio-demographic factors.
Demographic characteristics have shown that most of respondents were Chinese, and the majority were 35–50 years old. Among racial distribution, Chinese population ratio 152(45.10 %) was higher followed by Malays 137(40.65 %) and Indians 37(10.97 %). Besides that, 79.52 % have an average educational background, which is consistent with another study conducted in Malaysia [20]. The osteoporosis information, knowledge, understanding, and perception about exercise and calcium sources were poor (62.0 %). In line with our results, other studies show more than 50.0 % of patients have correct knowledge about exercise for bone health [19] and, therefore, require preventive educational training programs to increase awareness about osteoporosis [21], [22], [23]. Poor knowledge among current study participants depicts a low perception of seriousness towards osteoporosis. Although knowledge is a crucial component in promoting self-care, knowledge alone still cannot result in the practice of preventive behavior or a positive attitude [24]. So, it is necessary to perceive the seriousness of osteoporosis among TB patients. Literature has shown that people believe osteoporosis is an inevitable factor of ageing and do not take it as a severe disease that may even cause death [25], [26]. In the case of osteoporosis knowledge among TB patients, the results of our study indicate that 54.7 % of total females had good knowledge on osteoporosis than males (Fig. 1), which is consistent with an Indian study where women were reported to had higher knowledge than men [27]. While males had significantly poor knowledge score (OR 3.86, 95 % CI 1.98–7.53), which would be explained by postulating that osteoporosis in men is a relatively unknown topic and has been described rarely. The osteoporotic fracture risk in men is roughly one-third of women, but the fatality risk following the fracture is 1.6 times higher in men [15].
TB patients with poor knowledge of osteoporosis indicated that majority of participants were not well educated. Study participants with no formal education (OR 4.34, 95 % CI 1.11–16.84) or ≤12 years of education (OR 3.63, 95 % CI 1.52–8.65) were significantly responsible for poor OKT scores (Table 3). Patients with >12 years of education have a good proportion of knowledge, supporting our finding that educational level was reported as a significant factor in a few studies [28], [29]. Furthermore, rural residents had been associated with low knowledge of osteoporosis [30]. In line with the present study, rural residency (OR 2.49, 95 % CI 1.46–4.27) significantly influences the unawareness of osteoporosis knowledge among TB patients [21]. This could be because , the training campaigns for disease awareness are mainly carried out in the megacity or overpopulated areas in developing countries. This practice might become the decisive reason for the low level of knowledge in rural areas. In our results, a significant association was found between low-income level (OR 1.92, 95 % CI 1.12–3.30) and poor knowledge of osteoporosis (Table 3), as supported by the literature [11], [31].
The findings of this study strongly indicate the need to develop policies and conduct community-based programs mainly focused on increasing public awareness and knowledge of the disease. Critical interventions are compulsory to improve attitudes towards osteoporosis among TB patients. On observing the rising trend of osteoporosis in different age groups, it is necessary to enhance the role of general physicians to raise awareness regarding osteoporosis at various health clinics and centres. Current study findings can be used as scientific evidence to help design and provide adequate health education.
A limitation inherent in most knowledge assessment studies is the cross-sectional study design and sampling techniques that could have created some bias. We conducted this study with limited resources. Future studies must include a more extensive sample of TB patients from different health centres and tertiary hospitals in Pinang to explore more accurate and in-depth results. In addition, future studies are needed to shed light on daily practices of patient exertion and nutritional approaches, such as protein and calcium intake, to avoid more health complications.
Conclusion
5
Overall, TB patients had poor osteoporosis knowledge. Implementing awareness and educational programs among TB patients might increase preventive practices and measures toward osteoporosis. Such preventive procedures need to focus on calcium-rich nutrition and regular exercise.
Availability of data and materials
The datasets used and analyzed during the current study available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Funding
No funding.
Ethical approval
The study was approved by the Medical Research Ethics Committee (MREC), Ministry of Health, and Malaysia (Registration ID: NMRR-18-1145-40397; MREC reference: dim. KKM/NIHSEC P18-1198(6).
Authors contribution
Zohra Bhatti: Conceptualization, Methodology, Investigation, Writing-original draft, Data Curation, Formal analysis, Investigation Madeeha Laghari Conceptualization, Methodology, Writing- review and editing, Visualization. Amer Hayat Khan supervised this project. Conceptualization, Project administration, Investigation, Supervision, Validation. Syed Azhar Syed Sulaiman Project administration, Resources, Supervision. Bandeh Ali Talpur Formal analysis, Funding acquisition. Software, Validation.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Subramaniam S.Chan C.-Y.Soelaiman I.-N.Mohamed N.Muhammad N.Ahmad F.Prevalence and predictors of osteoporosis among the chinese population in Klang Valley, Malaysia Appl Sci 9920191820
- 2Chin K.-Y.Kamaruddin A.A.A.Low N.Y.Ima-Nirwana S.Effects of age, sex, and ethnicity on bone health status of the elderly in Kuala Lumpur, Malaysia Clin Interv Aging 1120167677732735855810.2147/CIA.S 108772 PMC 4912315 · doi ↗ · pubmed ↗
- 3IOF. Asia Pacific Audit Malaysia. 2013 https://www.iofbonehealth.org/sites/default/files/media/PD Fs/Regional%20Audits/2013-Asia_Pacific_Audit-Malaysia_0_0.pdf.
- 4Holloway K.L.Link K.Rühli F.Henneberg M.Neyrolles O.Skeletal lesions in human tuberculosis may sometimes heal: an aid to palaeopathological diagnoses P Lo S One 84201310.1371/journal.pone.0062798 PMC 363476323638146 · doi ↗ · pubmed ↗
- 5Yeh J.-J.Wang Y.-C.Lin C.-C.Lin C.-L.Hsu W.-H.Nguyen T.V.Association of respiratory tuberculosis with incident bone fracture: bridging the tuberculosis airway infection and the osteoporotic bone P Lo S One 1112201610.1371/journal.pone.0168673 PMC 517899728005963 · doi ↗ · pubmed ↗
- 6Chen Y.-Y.Feng J.-Y.Ting W.-Y.Yen Y.-F.Chuang P.-H.Pan S.-W.Increased risk of incident osteoporosis and osteoporotic fracture in tuberculosis patients: a population-based study in a tuberculosis-endemic area Osteoporos Int 2852017171117212833196610.1007/s 00198-017-3939-x · doi ↗ · pubmed ↗
- 7Choi C.-J.Choi W.-S.Kim C.-M.Lee S.-Y.Kim K.-S.Risk of sarcopenia and osteoporosis in male tuberculosis survivors: korea national health and nutrition examination survey Sci Rep 712017131272903056010.1038/s 41598-017-12419-y PMC 5640648 · doi ↗ · pubmed ↗
- 8Nadler M.Alibhai S.Catton P.Catton C.To M.J.Jones J.M.Osteoporosis knowledge, health beliefs, and healthy bone behaviours in patients on androgen-deprivation therapy (ADT) for prostate cancer BJU Int 11182013130113092335106210.1111/j.1464-410X.2012.11777.x · doi ↗ · pubmed ↗