Chronic Inflammatory Demyelinating Polyneuropathy as the Initial Presentation of Systemic Lupus Erythematosus Successfully Treated With Cyclophosphamide
Andrés D Sastre Martínez, María J Tróchez Ortiz, Lizeth V Zuluaga Gómez, Christian D Messu Llano

TL;DR
A rare case of lupus initially presenting as a nerve disorder was successfully treated with cyclophosphamide and steroids.
Contribution
Highlights a unique treatment approach for CIDP as the initial manifestation of SLE.
Findings
CIDP can be the first sign of SLE, complicating early diagnosis.
Cyclophosphamide and steroids provided a favorable outcome in this case.
More research is needed to guide treatment for CIDP in SLE patients.
Abstract
Systemic lupus erythematosus (SLE) is an autoimmune disorder that can manifest with a wide range of clinical features, including peripheral nervous system involvement. Among the neurological complications associated with SLE, chronic inflammatory demyelinating polyneuropathy (CIDP) is a rare but significant entity. This case report explores the complex relationship between CIDP and SLE, emphasizing the challenges in diagnosis and the complexities of treatment strategies. We present the case of a patient diagnosed with CIDP as the initial manifestation of SLE, who exhibited a remarkable response to a unique treatment approach. This case underscores the potential overlap of these two conditions, the need for individualized diagnostic, and the importance of considering lupus activity when making therapeutic decisions. While conventional treatment approaches for CIDP are established, the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
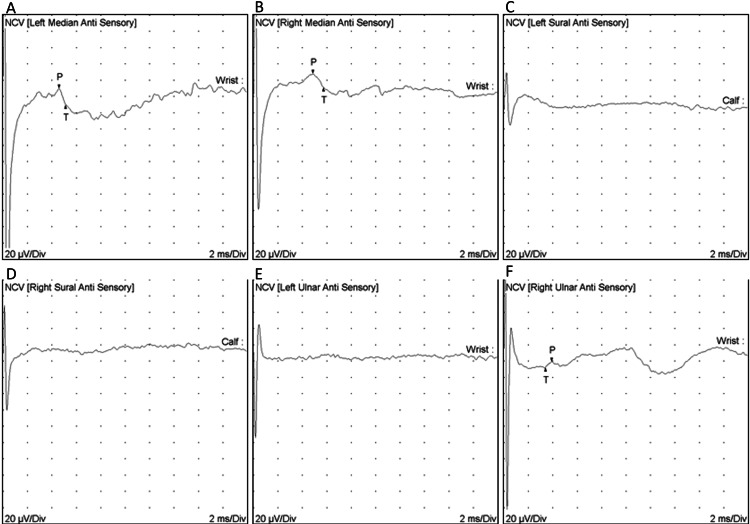 Figure 1
Figure 1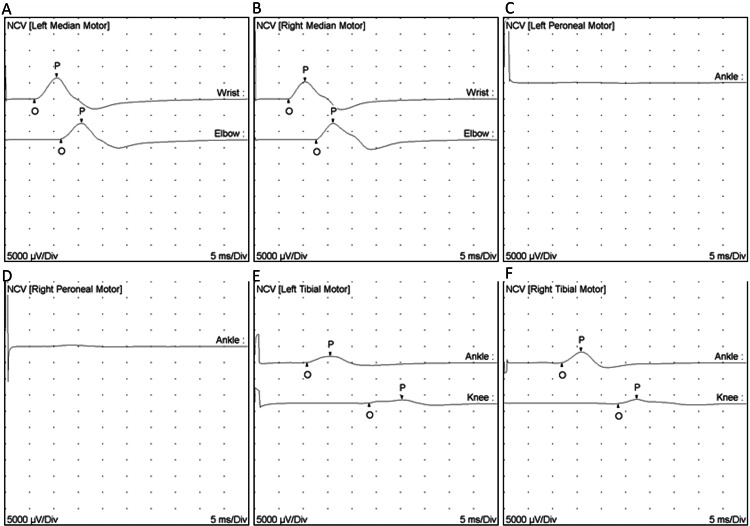 Figure 2
Figure 2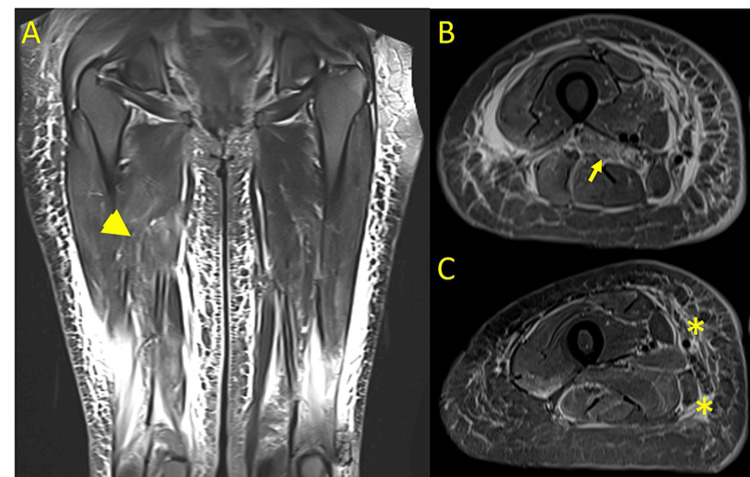 Figure 3
Figure 3| Test | Result | Reference range |
| Opening pressure | 13 cm H2O | < 20 cm H20 |
| Appearance | Clear, colorless | Clear |
| Glucose | 63 mg/dl | 50-80 mg/dl |
| Proteins | 300 mg/dl | < 45 mg/dl |
| Red blood cells | 250 cells/mm3 | < 5 cells/mm3 |
| White blood cells | 0 cells/mm3 | < 5 cells/mm3 |
| Lymphocytes | 0 cells/mm3 | < 5 cells/mm3 |
| Mononuclear cells | 0 cells/mm3 | < 5 cells/mm3 |
| Lactate dehydrogenase | < 41 IU/l | < 41 IU/l |
| Gram stain | No leukocytes or bacteria | |
| KOH stain | Negative for yeast | |
| Ziehl-Neelsen stain | Negative for AFB | |
| Bacteria culture | Negative | |
| Fungus culture | Negative | |
| Mycobacteria culture | Negative | |
| Test | Result | Reference range |
| Leukocyte count | 4.68 x 103 cells/mm3 | 3.98-10.04 x 103 cells/mm3 |
| Neutrophil count | 3.62 x 103 cells/mm3 | 1.56-6.13 x 103 cells/mm3 |
| Lymphocyte count | 0.85 x 103 cells/mm3 | 1.18-3.74 x 103 cells/mm3 |
| Hemoglobin | 12.8 g/dl | 11.2-15.7 g/dl |
| Platelet count | 368 x 103 cells/mm3 | 182-369 x 103 cells/mm3 |
| Total serum proteins | 5.24 g/dl | 6.3-8.2 |
| Albumin | 1.8 g/dl | 3.5-5 g/dl |
| Creatinine | 0.6 mg/dl | 0.52-1.04 mg/dl |
| Creatine kinase | 169 IU/l | 30-135 IU/l |
| C-reactive protein | 5 mg/dl | < 9.99 mg/dl |
| Erythrocyte sedimentation rate | 57 mm/h | 1-20 mm/h |
| Total cholesterol | 288 mg/dl | 0-200 mg/dl |
| LDL cholesterol | 146 mg/dl | < 130 mg/dl |
| Triglycerides | 328 mg/dl | 0-150 mg/dl |
| Complement C3 | 61 mg/dl | 88-165 mg/dl |
| Complement C4 | 8.4 mg/dl | 14-44 mg/dl |
| Antinuclear antibodies | 1:1280 fine speckled pattern | |
| Extractable nuclear antibodies | Negative | Negative |
| Anti-DNA antibodies | Non-reactive | Non-reactive |
| IgM anticardiolipin antibodies | 0.9 MPL-U/ml | < 10 MPL-U/ml |
| IgG anticardiolipin antibodies | 1.6 GPL-U/ml | < 10 GPL-U/ml |
| IgM anti-B2 glycoprotein antibodies | 0.9 IU/ml | < 5 IU/ml |
| IgG anti-B2 glycoprotein antibodies | 2.8 IU/ml | < 5 IU/ml |
| Lupus anticoagulant ratio screening | 0.9 | < 1.2 |
| Anti-Jo1 antibodies | 1.7 IU/ml | < 15 IU/ml |
| HIV antibodies | Negative | Negative |
| VDRL | Non-reactive | Non-reactive |
| TPPA | 0.01 | < 0.08 |
| Hepatitis B surface antigen | Negative | Negative |
| Hepatitis C total antibodies | Negative | Negative |
| HTLV I-II antibodies | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Hereditary Neurological Disorders · Systemic Lupus Erythematosus Research
Introduction
Systemic lupus erythematosus (SLE) is a chronic connective tissue disease that affects multiple systems and organs. Neurological involvement is common, and the term "neuropsychiatric lupus" has been proposed to encompass the neurologic manifestations [1], including central and peripheral nervous system involvement, with neuropathies being one of the most common forms of presentation [2]. Chronic inflammatory demyelinating polyneuropathy (CIDP) is a clinical condition characterized by progressive weakness and sensory loss mediated by an immune response. It is possible that CIDP may be the initial clinical manifestation of lupus [3,4]. Initial treatment typically involves corticosteroids, intravenous immunoglobulin (IVIG), or plasma exchange. However, other immunomodulators such as rituximab, cyclosporine, or cyclophosphamide may be considered [5]. Here, we present the case of a patient with a CIDP diagnosis as the initial manifestation of SLE, who experienced satisfactory improvement following treatment with intravenous (IV) steroids and cyclophosphamide.
Case presentation
A 32-year-old woman of African descent, with no relevant past medical history, presented to the emergency department due to two months of progressive leg weakness leading to walking difficulties. The patient also reported paresthesia in her fingers and the soles of her feet. Over time, the weakness and paresthesia extended to the upper limbs. She also complained about joint pain in her fingers, generalized hair loss, swelling in the lower limbs, and unintentional weight loss over the last six months.
Brain and cervical-thoracic-lumbar spinal cord magnetic resonance imaging ruled out central nervous system involvement. A lumbar puncture demonstrated albumin-cytologic dissociation, and central nervous system infections were excluded (Table 1).
Due to systemic symptoms, biochemical studies and autoimmunity tests were conducted, revealing high-titer positive antinuclear antibodies (ANA), consumption of complement C3 and C4, hyperlipidemia, severe hypoalbuminemia, and proteinuria. The extractable nuclear antigen (ENA) test was negative, and tests for human immunodeficiency virus (HIV), syphilis, hepatitis B, hepatitis C, and human T-cell lymphotropic virus (HTLV) infections were all negative (Table 2).
A progressive chronic peripheral neuropathy was suspected, and nerve conduction studies of the four limbs were performed revealing a chronic demyelinating motor and sensory polyneuropathy with secondary axonal changes (Figure 1 and Figure 2).
Sensory nerve conduction study. A. Left median anti-sensory. B. Right median anti-sensory. C. Left sural anti-sensory. D. Right sural anti-sensory. E. Left ulnar anti-sensory. F. Right ulnar anti-sensory.The left and right median nerves (Panels A and B), as well as the right ulnar nerve (Panel F), show prolonged distal latency and decreased conduction velocity. Both the left and right sural nerves (Panels C and D) and the left ulnar nerve (Panel E) lack excitability.
Motor nerve conduction study. A. Left median motor. B. Right median motor. C. Left peroneal. D. Right peroneal. E. Left tibial motor. F. Right tibial motor.Both the left and right median nerves (Panels A and B), along with the left and right tibial nerves (Panels E and F), exhibit prolonged distal latency and reduced conduction velocity. The left and right peroneal nerves (Panels C and D) are non-excitable.
Total creatine kinase (CK) levels were slightly elevated upon admission, so a lower limb magnetic resonance imaging was performed which showed diffuse muscle edema with predominant involvement in the quadriceps, confirming myositis (Figure 3).
Lower limb magnetic resonance imaging.A. Contrast-enhanced T2 coronal view of both thighs. There's muscle edema predominantly in the right quadriceps (arrowhead). B. Contrast-enhanced T1 TIRM view of the left thigh showing muscle edema (arrow). C. Contrast-enhanced T2 view of the left thigh showing edema in the middle muscle compartment and subcutaneous tissue (asterisk).TIRM: turbo inversion recovery magnitude
A 24-hour urine collection revealed massive proteinuria of 20,235 mg, confirming nephrotic syndrome. A kidney biopsy was performed, and pathology showed a generalized increase in cellularity in the mesangial area, endocapillary proliferation, and infiltration by mixed inflammatory cells. No signs of sclerosis or structural alterations were found in the glomeruli or renal interstitium. The analyzed arterial vessels showed no abnormalities. Immunofluorescence samples revealed no identified glomeruli in the preparation, and there was no positive staining observed in tubules or vessels. The specimen was conclusive for proliferative mesangial glomerulonephritis, with the absence of immune complex deposits in the examined tissues.
Considering these findings, the diagnosis of SLE was confirmed, supported by peripheral nervous system involvement as evidenced by chronic demyelinating polyneuropathy, muscle involvement attributable to myositis, and class II lupus nephritis. Due to multisystemic involvement, particularly with renal compromise, treatment was initiated with 500 mg IV methylprednisolone pulses for three days, followed by cyclophosphamide at a dose of 750 mg/m^2^ every month for six doses, tapering prednisone, hydroxychloroquine, vitamin D, and physical therapy. Additionally, atorvastatin was initiated for secondary dyslipidemia and losartan as an anti-proteinuric measure, and warfarin was the patient's preferred choice for anticoagulation due to the risk of venous thrombosis associated with massive proteinuria and severe hypoalbuminemia.
After two months, the patient has shown significant improvement. Although she still experiences mild weakness, predominantly in the proximal lower limbs, she can walk and move independently. Serum albumin levels haven't changed, but 24-hour proteinuria improved to 6,574 mg.
Discussion
Peripheral nervous system involvement in SLE can manifest as multiple mononeuritis, autoimmune necrotizing myopathy, autonomic neuropathy, myasthenia gravis, peripheral neuropathy, and demyelinating inflammatory polyneuropathy in the acute (AIDP) or chronic (CIDP) spectrum. These last two conditions are rare complications, occurring in as few as 0.8% of patients [1,2]. CIDP may occur simultaneously with lupus, or CIDP may precede or follow the onset of SLE [3].
CIDP is a macrophage-mediated disorder resulting from dysregulated immune response, developing over at least eight weeks. It is characterized by axonal damage and demyelination of peripheral nerves [4]. The evaluation of this condition is based on clinical manifestations, electrophysiological studies, and supportive tests such as cerebrospinal fluid analysis to confirm elevated protein levels with little to no pleocytosis [4,5]. Other diagnostic tools include magnetic resonance imaging of the cervical or lumbar plexus, ultrasound, or peripheral nerve biopsy, to differentiate between defined and possible CIDP [5].
The pathogenesis of the association between these two conditions is not clearly defined, but it is believed to involve both cellular and humoral immunity, leading to neurogenic inflammation resulting in axonal or myelin damage due to autoantibodies against nodal and extranodal structures, given the high number of antigens at the Ranvier node [6,7]. Anti-ganglioside antibodies have been described in 15-24% of patients with peripheral nervous system involvement in SLE. However, some studies did not show an association with antinuclear antibodies, anti-DNA antibodies, antiphospholipid antibodies, or low complement levels [6-9]. It is now understood that CIDP can be an autoimmune condition in its own, sharing certain HLA loci and common mechanisms with other autoimmune diseases [3].
Current guidelines for CIDP treatment recommend initiating oral or pulse corticosteroids, IVIG/subcutaneous immunoglobulin (SCIG), or plasma exchange, either alone or in combination, based on clinical response [5]. In cases of refractoriness, after assessing risks and benefits, unconventional therapies such as cyclophosphamide, rituximab, or even autologous hematopoietic stem cell transplantation may be considered [5,10]. However, the management of CIDP in patients with SLE differs from the standard approach. Conventionally, steroids have been used in combination with IVIG, as in the characterization by Julio et al., where 13 out of 16 patients received it. Nonetheless, these authors suggest that the initial treatment should be determined by the activity of SLE. In the absence of lupus activity, treatment should follow the current CIDP treatment guidelines. When lupus activity is present, corticosteroids can be combined with immunomodulators such as cyclophosphamide or rituximab. If there is no response, the initiation of IVIG/SCIG should be considered [11]. Currently, there are no clinical trials evaluating this approach, and case reports of successful treatment with immunomodulators before IVIG or plasma exchange are limited [11,12]. In the case presented here, a favorable response to initial treatment with steroids and cyclophosphamide is reported, without the addition of IVIG. This could be considered as a therapeutic alternative, especially in cases where multiple systems are involved and other manifestations like inflammatory myositis and lupus nephritis are present.
Conclusions
This case highlights the intricate interplay between CIDP and SLE. While the exact mechanisms linking these conditions remain unclear, a tailored approach is crucial for diagnosis and treatment. Treatment decisions should consider lupus activity, and this case highlights that early intervention with steroids and cyclophosphamide, in the absence of immediate IVIG or plasma exchange, can lead to favorable outcomes. Further research is needed to establish clear management guidelines for this unique patient subset, optimizing care while mitigating the risks associated with immunomodulatory therapies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Neurological complications in patients with systemic lupus erythematosus Curr Neurol Neurosci Rep Shaban A Leira EC 971920193177330610.1007/s 11910-019-1012-1 · doi ↗ · pubmed ↗
- 2Neuropsychiatric lupus: new mechanistic insights and future treatment directions Nat Rev Rheumatol Schwartz N Stock AD Putterman C 1371521520193065924510.1038/s 41584-018-0156-8PMC 8023338 · doi ↗ · pubmed ↗
- 3Chronic inflammatory demyelinating polyneuropathy as an autoimmune disease J Autoimmun Rodríguez Y Vatti N Ramírez-Santana C Chang C Mancera-Páez O Gershwin ME Anaya JM 83710220193107274210.1016/j.jaut.2019.04.021 · doi ↗ · pubmed ↗
- 4Chronic inflammatory demyelinating polyradiculoneuropathy-diagnostic pitfalls and treatment approach Muscle Nerve Stino AM Naddaf E Dyck PJ Dyck PJ 1571696320213291490210.1002/mus.27046 · doi ↗ · pubmed ↗
- 5European Academy of Neurology/Peripheral Nerve Society guideline on diagnosis and treatment of chronic inflammatory demyelinating polyradiculoneuropathy: report of a joint task force-second revision Eur J Neurol Van den Bergh PY van Doorn PA Hadden RD 355635832820213432776010.1111/ene.14959 · doi ↗ · pubmed ↗
- 6Peripheral nervous system involvement in systemic lupus erythematosus: a review of the evidence Clin Exp Rheumatol Bortoluzzi A Silvagni E Furini F Piga M Govoni M 146155372019 https://pubmed.ncbi.nlm.nih.gov/29846158/29846158 · pubmed ↗
- 7Peripheral neuropathies in systemic lupus erythematosus: clinical features, disease associations, and immunologic characteristics evaluated over a twenty-five-year study period Arthritis Rheumatol Oomatia A Fang H Petri M Birnbaum J 100010096620142475715110.1002/art.38302 · doi ↗ · pubmed ↗
- 8Peripheral neuropathy in patients with systemic lupus erythematosus Semin Arthritis Rheum Florica B Aghdassi E Su J Gladman DD Urowitz MB Fortin PR 2032114120112164101810.1016/j.semarthrit.2011.04.001 · doi ↗ · pubmed ↗