Coronary artery haematoma after primary percutaneous coronary intervention: late, trans-stent, retrograde progression
Yoshihiro Harano, Yoshiaki Kawase, Hitoshi Matsuo

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
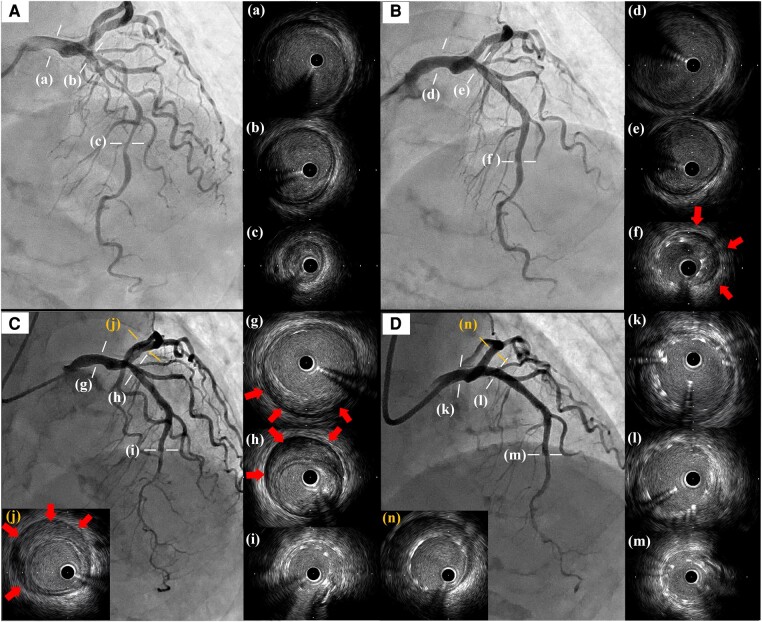 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Kawasaki Disease and Coronary Complications · Acute Myocardial Infarction Research
One of the common complications of percutaneous coronary intervention (PCI) is iatrogenic coronary intramural haematoma (CIH), which sometimes worsens in the days following the PCI.^1^
A 73-year-old woman was transferred to our hospital due to unstable angina. Initial coronary angiography showed a severe lesion in the middle of the left anterior descending artery (LAD), and intravascular ultrasound study (IVUS) revealed a low-echoic plaque but no haematoma at the lesion (Figure 1A). Emergent PCI was performed by implantation of a 2.5 × 38 mm drug-eluting stent (DES) followed by post-dilation with a 3.0 × 12 mm non-compliant balloon at the stent proximal zone. The presence of CIH at the distal end of the stent was subsequently demonstrated on IVUS imaging (Figure 1B). Additional stenting was not performed as a subsequent IVUS conducted 15 min later showed no progression of the CIH. Due to the lack of complete recovery of the chest discomfort, the patient was closely followed in our hospital. On Day 7, the patient’s chest pain suddenly worsened and the electrocardiogram showed newly developed ST-segment elevation in the inferior leads. Emergent coronary angiography and IVUS demonstrated that the CIH had surprisingly progressed retrogradely beyond the implanted DES to the left main trunk (LMT) and the left circumflex artery (LCX) (Figure 1C). A bailout PCI was performed by covering the haematoma using a T-stent method: one 4.0 × 21 mm DES from the LMT to the proximal LAD and the other 3.5 × 18 mm DES in the proximal LCX (Figure 1D). Follow-up coronary computed tomographic angiography on the following day revealed no further progression of CIH.
Iatrogenic CIH occurred in 6.7% of patients after PCI and sometimes worsened in the days or weeks following the intervention.^1^ In this case report, we demonstrate how the haematoma can advance retrogradely even in the presence of an implanted stent.
Consent: The authors confirm that written consent for submission and publication of this case report, including images and associated text, has been obtained from the patient according to the COPE guidelines.
Funding: None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maehara A, Mintz GS, Bui AB, Castagna MT, Walter OR, Pappas C, et al Incidence, morphology, angiographic findings, and outcomes of intramural haematomas after percutaneous coronary interventions: an intravascular ultrasound study. Circulation 2002;105:2037–2042.11980682 10.1161/01.cir.0000015503.04751.bd · doi ↗ · pubmed ↗