The introduction of fluoroscopic surgery: A report of an initial trial case
Junji Takahashi, Masashi Yoshida, Teppei Kamada, Keigo Nakashima, Norihiko Suzuki, Yutaka Suzuki

TL;DR
This case report introduces a new fluoroscopic surgery technique using continuous ICG infusion to keep blood vessels visible without switching light modes.
Contribution
This is the first study to use continuously infused ICG during surgery.
Findings
Continuous ICG angiography allowed the appendiceal artery to remain visible throughout the operation.
The fluoroscopic surgery technique was feasible without switching to white light mode.
The method was successfully tested in an appendectomy as an initial trial.
Abstract
Switching from white light to fluorescence mode is necessary to confirm the fluorescence during fluorescence-guided surgery. This case report presents the use of a syringe pump to continuously inject indocyanine green (ICG), which enabled the vessels to be visualised and the operation to be performed without switching. An Asian male patient in his 40s underwent an interval appendectomy following conservative treatment for appendicitis. Laparoscopic surgery was performed using the VISIONSENSE® system. Diluted ICG (25 mg/15 mL) was intravenously administered at 1 mL/min. The appendiceal artery was visualised in light green, and the intensity of the visualisation was defined relative to the tissue surrounding the dissected appendiceal artery. The superior rectal artery and the vessels within the mesentery of the small intestine were confirmed to be continuously visualised throughout the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1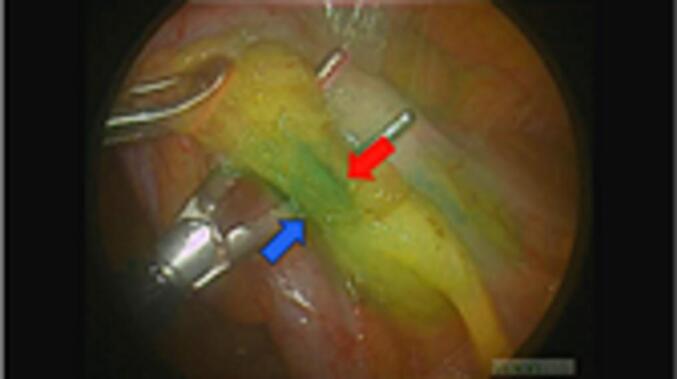 Figure 2
Figure 2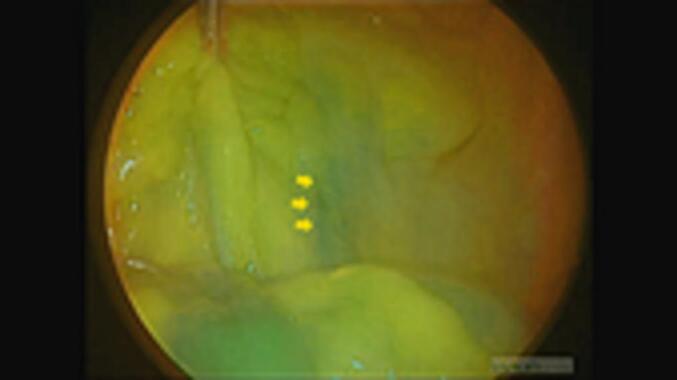 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMinimally Invasive Surgical Techniques · Colorectal Cancer Surgical Treatments · Breast Implant and Reconstruction
Introduction
1
The surgical procedure that uses the advantage of fluorescence is known as “fluorescence-guided surgery”. Switching from white light to fluorescence mode is necessary during fluorescence-guided surgery to confirm the fluorescence. In such cases, the surgical procedure is stopped while confirming the fluorescence. However, the development of the bright field full-colour fluoroscope enabled us to perform indocyanine green (ICG) fluorescence-guided laparoscopic cholecystectomy without switching to white light mode, and we reported the first case [1]. Therefore, this type of fluorescence-guided surgery without switching to the white light mode was termed “fluoroscopic surgery”.
The use of ICG fluorescence techniques for intraoperative vessel visualisation has been suggested as a valuable technique in neurosurgery and reconstructive surgery [2,3]. Moreover, its utility has been reported in gastric and colorectal cancer surgeries to identify the subpyloric artery [4] and target vessels [5], respectively. Typically, ICG is administered through a single intravenous bolus injection, making arteries visible within 1 min.
However, an obstacle to performing fluoroscopic surgery for vascular and blood flow recognition was the rapid disappearance of ICG from the blood flow. Approximately 90 % of ICG disappears from the blood flow within 15 min, and the arteries are only clearly visualised in the first 30 s [6].
Therefore, to resolve this challenge, we attempted to administer ICG continuously using a syringe pump. The first trial of this new fluoroscopic surgery using a syringe pump was applied in this case of appendectomy, a procedure usually completed within 1 h.
This report was prepared in accordance with the SCARE 2023 criteria [7].
Presentation of case
2
An Asian male patient in his 40s with diabetes mellitus (glycated haemoglobin level of 7.7 %) and chronic renal failure underwent treatment with dialysis. Two months after conservative appendicitis treatment, the patient underwent an interval appendectomy with laparoscopic surgery performed by a resident physician.
The VISIONSENSE® laparoscopic system (Medtronic, Dublin, Ireland) was employed in this laparoscopic surgery. However, we did not use the threshold-adjustment function of this system to discard the near-infrared signal or the infrared boost function. Diluted ICG of 25 mg/15 mL was administered intravenously using a syringe pump at 1 mL/min and continued for 7.7 min until the end of the vascular dissection (Fig. 1).Fig. 1. Blood vessels are continuously illuminated in green. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)Fig. 1
The appendiceal artery was visualised in light green and was clipped and dissected with an energy device for 1.67 min (Fig. 1). The appendiceal vein appeared darker green than the appendiceal artery, and the visualisation intensity was defined relative to the tissue surrounding the dissected appendiceal artery.
Subsequently, we ligated the appendiceal vein at the level of the appendiceal root and dissected it using an energy device (Fig. 2). The appendix was removed and assessed for intra-abdominal bleeding. Simultaneously, the superior rectal artery and the vessels within the mesentery of the small intestine were confirmed to be continuously visualised under fluorescent angiography (Fig. 3, Fig. 4). The total operative time was 56 min, with 5 g of blood loss; however, no intraoperative complications were observed. Finally, the patient was subsequently discharged from the hospital uneventfully 2 days after surgery.Fig. 2. The appendiceal vein (blue arrow) appeared darker green than the appendiceal artery (red arrow). (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)Fig. 2. Fig. 3The superior rectal artery (orange arrows) was confirmed to be continuously visualised throughout the surgery.Fig. 3. Fig. 4The vessels within the mesentery of the small intestine (red arrow) were verified as fluorescent through to the end of the operation. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)Fig. 4
Discussion
3
This is the first report of fluoroscopic surgery of the gastrointestinal tract.
The concept of fluoroscopic surgery was inspired by the development of fluorescent cameras, which were initially launched as monochrome cameras [8] and later advanced to full colour, applied to laparoscopy, and advanced to dichromatic [9]. Currently, fluorescent laparoscopic cameras are equipped with bright-field and full-colour capabilities [10], including the recently developed high-definition technology. Therefore, using this continuously fluorescing device, we could assess what exhibits fluorescence and what does not and reach a level where surgery may be improved by viewing fluorescent images.
In this case, the continuous ICG angiography enabled us to operate while keeping the appendiceal artery visible. Continuous ICG angiography for the location of vessels can be performed even when the intestinal tract is moved, allowing surgery to be performed with a constant awareness of the artery's location, including unexpected anomalies. The tissue around the vessel was successfully dissected while outlining the vessel diameter, potentially reducing the risk of accidental vessel injury.
This initial demonstration of continuous ICG angiography shows that continuous ICG can be used instead of a single intravenous bolus injection. Furthermore, since we could continuously observe the superior mesenteric artery and small mesenteric vessels, it also provides the possibility that this method can be applied to other areas of surgery in the future.
However, since this is only one case, it should be noted that visibility may be insufficient in cases with a thick mesangial fat layer; therefore, a case series should be conducted to examine the efficacy of this method in several types of surgery.
Conclusion
4
The fluoroscopic surgery using a syringe pump without switching to white light mode was feasible in this first case report.
Informed consent
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Ethical review was not required for this case report as it was a study using an existing drug and a single case report.
Funding
We have no sponsors.
Author contribution
JT: study design, data collection, data analysis, writing.
MY: critical revision
YS: final approval of the article
Any other authors: study design, data collection
All authors read and approved the final manuscript.
Guarantor
Junji Takahashi, the corresponding author of this manuscript accept full responsibility for the work and the conduct of the study, access to the data and controlled the decision to publish.
Research registration number
This paper is case report. The authors don’t need to register this work.
Conflict of interest statement
There are no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Takahashi J.Yoshida M.Nakaseko Y.Nakashima K.Kamada T.Suzuki N.Laparoscopic cholecystectomy completely guided by indocyanine green fluorescence in a patient with gallstone: a case report Int. J. Surg. Case Rep.88202110653310.1016/j.ijscr.2021.106533 PMC 857746034741854 · doi ↗ · pubmed ↗
- 2Raabe A.Beck J.Gerlach R.Zimmermann M.Seifert V.Near-infrared indocyanine green video angiography: a new method for intraoperative assessment of vascular flow Neurosurgery 5220031321391249311010.1097/00006123-200301000-00017 · doi ↗ · pubmed ↗
- 3Komorowska-Timek E.Gurtner G.C.Intraoperative perfusion mapping with laser-assisted indocyanine green imaging can predict and prevent complications in immediate breast reconstruction Plast. Reconstr. Surg.1252010106510732033585910.1097/PRS.0b 013e 3181 d 17f 80 · doi ↗ · pubmed ↗
- 4Ryu S.Suwa K.Kitagawa T.Aizawa M.Ushigme T.Okamoto T.Real-time fluorescence vessel navigation using indocyanine green during laparoscopic colorectal cancer surgery Anticancer Res 392019300930133117714210.21873/anticanres.13433 · doi ↗ · pubmed ↗
- 5Kim M.Son S.Y.Cui L.H.Shin H.J.Hur H.Han S.U.Real-time vessel navigation using indocyanine green fluorescence during robotic or laparoscopic gastrectomy for gastric cancer J. Gastric. Cancer 1720171451532868071910.5230/jgc.2017.17.e 17PMC 5489543 · doi ↗ · pubmed ↗
- 6Kamada T.Ohdaira H.Nakashima K.Nishide R.Nishie R.Takahashi J.Real-time vessel navigation using indocyanine green fluorescence during robotic-assisted gastrectomy for gastric cancer after coronary artery bypass grafting using the right gastroepiploic artery Asian J. Endoscop. Surg 16202353353610.1111/ases.1316136599190 · doi ↗ · pubmed ↗
- 7Sohrabi C.Mathew G.Maria N.Kerwan A.Franchi T.Agha R.A.The SCARE 2023 guideline: updating consensus surgical C Ase R Eport (SCARE) guidelines Int. J. Surg. Lond. Engl.10952023113610.1097/JS 9.0000000000000373 PMC 1038940137013953 · doi ↗ · pubmed ↗
- 8Tagaya N.Shimoda M.Kato M.Nakagawa A.Abe A.Iwasaki Y.Intraoperative exploration of biliary anatomy using fluorescence imaging of indocyanine green in experimental and clinical cholecystectomies J. Hepatobiliary Pancreat. Sci.1720105956001980629910.1007/s 00534-009-0195-2 · doi ↗ · pubmed ↗