Trajectory of Healthcare Contact Days for Veterans With Advanced Gastrointestinal Malignancy
Whitney V Johnson, Quan H Phung, Vishal R Patel, Alexander K Tsai, Nivedita Arora, Mark A Klein, Anders D Westanmo, Anne H Blaes, Arjun Gupta

TL;DR
This study examines how often veterans with advanced gastrointestinal cancer interact with healthcare outside their homes, revealing patterns that could help improve care delivery.
Contribution
The study introduces healthcare contact days as a practical measure to assess the burden of healthcare on patients' lives.
Findings
Patients spent one-third of their days in healthcare contact.
Healthcare contact days followed a U-shaped pattern over the course of illness.
Contact days varied by clinical and sociodemographic factors.
Abstract
How and where patients with advanced cancer facing limited survival spend their time is critical. Healthcare contact days (days with healthcare contact outside the home) offer a patient-centered and practical measure of how much of a person’s life is consumed by healthcare. We retrospectively analyzed contact days among decedent veterans with stage IV gastrointestinal cancer at the Minneapolis Veterans Affairs Healthcare System from 2010 to 2021. Among 468 decedents, the median overall survival was 4 months. Patients spent 1 in 3 days with healthcare contact. Over the course of illness, the percentage of contact days followed a “U-shaped” pattern, with an initial post-diagnosis peak, a lower middle trough, and an eventual rise as patients neared the end-of-life. Contact days varied by clinical factors and by sociodemographics. These data have important implications for improving care…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
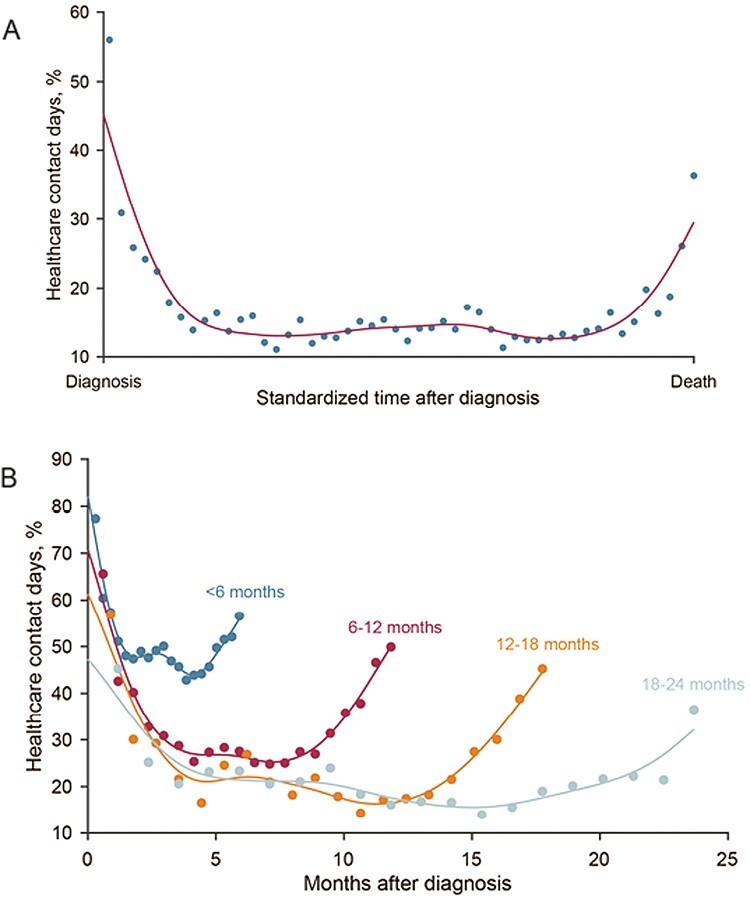 Fig. 1
Fig. 1| Patient characteristic | Data |
|---|---|
| Age at diagnosis in years, median (IQR) | 69 (64, 76) |
| Sex, Number (%) | |
| Male | 463 (98.9) |
| Female | 5 (1.1) |
| Charlson Score, median (IQR) | 2 [1, 3] |
| 70% or more service connected, number (%) | 94 (20.0) |
| Race, number (%) | |
| White | 387 (82.3) |
| Black or African American | 28 (6.0) |
| Native Hawaiian or Other Pacific Islander | 4 (0.9) |
| American Indian or Alaska Native | 4 (0.9) |
| Other/Unknown | 47 (10.0) |
| Ethnicity, number (%) | |
| Not Hispanic or Latino | 448 (95.3) |
| Hispanic or Latino | 3 (0.6) |
| Other/Unknown | 19 (4.0) |
| Rurality, number (%) | |
| Urban | 286 (60.9) |
| Rural | 183 (38.9) |
| Unknown | 1 (0.2) |
| Primary cancer location, number (%) | |
| Gastroesophageal | 146 (31.1) |
| Pancreatic | 133 (28.3) |
| Colorectal | 120 (25.5) |
| Hepatobiliary | 70 (14.9) |
| Other | 1 (0.2) |
| Year of diagnosis, number (%) | |
| 2010-2013 | 166 (35.3) |
| 2014-2017 | 143 (30.4) |
| 2018-2021 | 161 (34.3) |
| Receipt of any cancer-directed treatment, number (%) | 218 (46.6) |
| Ever hospitalized from diagnosis to death, number (%) | 413 (88.2) |
| Ever received care in emergency department, number (%) | 306 (65.8) |
- —Minnesota Colorectal Cancer Research Foundation
- —Pancreas Cancer Action Network
- —Institutional Research Grant
- —American Cancer Society10.13039/100000048
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth, Education, and Physical Culture · Educational and Social Studies · Italian Literature and Culture
Background
Patients with stage IV gastrointestinal cancer have healthcare needs related to the underlying cancer, receipt of and recovery from cancer-directed treatment, and management of comorbidities. This care is often essential but can also end up consuming patients’ lives, especially when uncoordinated.^1^ We have previously developed and described a measure of these time burdens, healthcare contact days, which encompasses days with care received outside the patients’ residence.^1^ We have applied contact days as a clinical trial endpoint and as a real-world measure of patient burden.^2-4^
The Veterans Affairs (VA) Hospital is the largest integrated health system in the US. It serves a population with relatively higher comorbidity burden and lower socioeconomic status than a non-VA population.^5^ We sought to characterize the patterns of contact days experienced by decedent veterans with stage IV gastrointestinal cancer.
Methods
We conducted a retrospective cohort analysis using the VA Clinical Cancer Registry (VACCR) and Corporate Data Warehouse (CDW) to identify decedents aged 18 years or older with stage IV gastrointestinal cancer (gastroesophageal, pancreatic, hepatobiliary, or colorectal) between 2011 and 2021 who received primary oncologic care at the Minneapolis VA Hospital, Minnesota, USA.^6^ Patients could receive additional community care.
We marked each day of follow-up (diagnosis to death) as a contact day (any day with contact with the healthcare system outside the home regardless of the duration or purpose) or a home day. If multiple healthcare encounters occurred on the same day (eg, outpatient labs, imaging, clinician visit), it was considered a single contact day but was counted within each source. We calculated overall percentage of contact as days contact days divided by overall survival.
To demonstrate the trajectory of contact days over the course of illness, we standardized the time from diagnosis to death (x-axis) and calculated a cubic smoothing spline to plot percentage contact days over time (Fig. 1A). We hypothesized that trajectories could vary by survival and thus also plotted trajectories after grouping patients into survival cohorts (0-6 months, 6-12 months, etc.) (Fig. 1B).
Percent of contact days from diagnosis to death for decedents with stage IV gastrointestinal malignancies for entire cohort (A), and grouped by duration of overall survival (B).
Using multivariable beta regression, we analyzed clinicodemographic factors associated with percentage of contact days and reported these as adjusted odds ratios with 95% confidence intervals. The Minneapolis VA institutional review board reviewed the project and determined that it did not constitute human research.
Results
We included 468 patients with stage IV gastrointestinal cancers. The most common primary sites were gastroesophageal (31.1%) and pancreatic (28.3%). The median age at diagnosis was 69 years (Table 1). Twenty percent of patients were 70% or more service-connected, and they were entitled to additional benefits due to medical conditions that were caused or worsened by military service.^7^
The median (IQR) overall survival was 126 days (49-317). Less than half of patients (46.6%) received cancer-directed treatment. The median number and percentage of contact days were 44 days and 34.9%. Ambulatory visits were the most common source of contact days (61.4%). A majority (88.2%) of patients were hospitalized at least once, with a median 13 hospital days (Table 1, Supplementary Table S1).
The highest percentage of contact days occurred immediately after diagnosis (45%) and before death (32%) with a trough in the middle, forming a U-shaped curve (Fig. 1A). The “”U’’ was consistent across survival cohorts; the depth of the trough was deeper as survival increased (Fig. 1B).
Higher comorbidity index (aOR 1.09 [1.03-1.15]) and more recent diagnosis year (2014-2017, vs. 2010-2013, aOR 1.48 [1.1-1.99]) were associated with higher percentage of contact days. Conversely, rural residence (versus urban, OR 0.76 [0.59-0.97]) was associated with fewer percentage contact days (Supplementary Table S2).
Discussion
In this single VA center report of decedents with stage IV gastrointestinal cancer, patients had a median survival of 4 months and spent 1 in 3 days with healthcare contact. Contact days followed a U-shaped trajectory and varied by clinical and sociodemographic factors.
The median survival of 4 months, while disappointing, is comparable to other contemporary real-world cohorts.^4^ The survival must be interpreted in the context of the underlying population, almost 60% with advanced gastroesophageal and pancreatic cancer (associated with worse prognosis), less than half received cancer-directed treatment (reflecting underlying sickness and ineligibility for treatment), and only included decedents (excluding longer-term survivors). The relatively lower rate of stage IV colorectal cancer in the cohort may relate to protocolized colorectal cancer screening at the VA, more coordinated preventive services at the VA are associated with improved cancer survival.^8^ Strikingly, patients spent one in every 3 days receiving predominantly outpatient healthcare, with a survival measured in months, similar to patients with advanced gastrointestinal cancer in non-VA settings.^4^
The percentage of contact days over time followed a “U-shaped” trajectory, with a higher proportion post-diagnosis and at the end-of-life. This pattern likely reflects the initial healthcare needs when patients present (eg, with jaundice), and the workup including staging and multidisciplinary input. As patients approach the end-of-life, healthcare needs rise again. Notably, the “”U’’ persisted when patients were divided into survival cohorts, but with deeper troughs the longer people lived. These results confirm the novel U-shaped contact days trajectory described recently in non-VA settings,^4^ also seen for health system costs. Interventions addressing the peaks or upswings of the U-curve (eg, multidisciplinary coordinated care and proactive palliative care) could reduce unnecessary contact days.^9^
Due to the unique population and care delivery within the VA, the findings of this study might have limited generalizability. However, the comprehensive care and robust data collection at the VA provide a unique opportunity to capture contact days. We did not include days with only telehealth visits or home-based care in the contact days measure, and this underestimates the total days with actual healthcare contact. Contact days also represent access to oftentimes necessary care, and care must be taken to not blindly interpret fewer contact days as universally good, especially for rural residents, who already face barriers to care.^10^ We only included decedents, which might exclude some long-term survivors. We did not judge the appropriateness of a contact day, and additional work is necessary to optimize judicious delivery of high-quality care.
Supplementary Material
oyad313_suppl_Supplementary_TablesClick here for additional data file.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gupta A , Eisenhauer EA, Booth CM. The time toxicity of cancer treatment. J Clin Oncol. 2022;40(15):1611-1615. 10.1200/JCO.21.0281035235366 · doi ↗ · pubmed ↗
- 2Gupta A , Hay AE, Crump M, et al Contact days associated with cancer treatments in the CCTG LY 12 trial. Oncologist. 2023;28(9):799-803. 10.1093/oncolo/oyad 12837226534 PMC 10485297 · doi ↗ · pubmed ↗
- 3Gupta A , O’Callaghan CJ, Zhu L, et al Evaluating the time toxicity of cancer treatment in the CCTG CO 17 trial. JCO Oncol Pract. 2023;19(6):e 859-e 866. 10.1200/OP.22.0073736881786 PMC 10337749 · doi ↗ · pubmed ↗
- 4Patel VR , Ramesh V, Tsai AK, et al. Health care contact days experienced by decedents with advanced GI cancer. JCO Oncol Pract. 2023:OP 2300232. 10.1200/OP.23.00232 PMC 1066701537738532 · doi ↗ · pubmed ↗
- 5Agha Z , Lofgren RP, Van Ruiswyk JV, Layde PM. Are patients at Veterans Affairs medical centers sicker? A comparative analysis of health status and medical resource use. Arch Intern Med. 2000;160(21):3252-3257. 10.1001/archinte.160.21.325211088086 · doi ↗ · pubmed ↗
- 6Fihn SD , Francis J, Clancy C, et al. Insights from advanced analytics at the Veterans Health Administration. Health Aff (Millwood). 2014;33(7):1203-1211. 10.1377/hlthaff.2014.005425006147 · doi ↗ · pubmed ↗
- 7Chapter 2 Service Connected Disabilities: Federal Benefits for Veterans, Dependents, and Survivors. US Department of Veterans Affairs. Accessed Nov 14, 2023. https://www.va.gov/opa/publications/benefits_book/2023_Federal_Benefits_for_Veterans_Dependents_and_Survivors.pdf . Published 2023.
- 8Landrum MB , Keating NL, Lamont EB, et al. Survival of older patients with cancer in the Veterans Health Administration versus fee-for-service Medicare. J Clin Oncol. 2012;30(10):1072-1079. 10.1200/JCO.2011.35.675822393093 PMC 3341151 · doi ↗ · pubmed ↗