Autoantibodies neutralizing GM-CSF in HIV-negative Colombian patients infected with Cryptococcus gattii and C. neoformans
Carlos A. Arango-Franco, Julián Rojas, Carolina Firacative, Clara Inés Agudelo, José Luis Franco, Jean-Laurent Casanova, Anne Puel, Jairo Lizarazo, Elizabeth Castañeda, Andrés A. Arias

TL;DR
Some Colombian patients with cryptococcosis have autoantibodies that block GM-CSF, a finding more common in those infected with Cryptococcus gattii.
Contribution
This study identifies a high prevalence of GM-CSF-neutralizing autoantibodies in HIV-negative Colombian patients with cryptococcosis, particularly those infected with C. gattii.
Findings
Autoantibodies neutralizing GM-CSF were detected in 69% of patients infected with C. gattii.
Only 6% of patients infected with C. neoformans had GM-CSF-neutralizing autoantibodies.
Nine out of ten patients with these autoantibodies were infected with C. gattii.
Abstract
Cryptococcosis is a life-threatening disease caused by Cryptococcus neoformans or C. gattii. Autoantibodies (auto-Abs) neutralizing granulocyte-macrophage colony-stimulating factor (GM-CSF) in otherwise healthy adults with cryptococcal meningitis have been described since 2013. We searched for neutralizing auto-Abs in sera from Colombian patients with non-HIV related cryptococcosis in a retrospective national cohort collected from 1997 to 2016. We reviewed clinical and laboratory records and assessed the presence of neutralizing auto-Abs in 30 HIV (−) adults presenting cryptococcosis (13 by C. gattii, and 17 by C. neoformans). We detected auto-Abs neutralizing GM-CSF in the plasma of 9 out of 13 (69%) patients infected with C. gattii and 1 out of 17 (6%) patients with C. neoformans. We report ten Colombian patients with cryptococcosis due to auto-Abs neutralizing GM-CSF. Nine of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
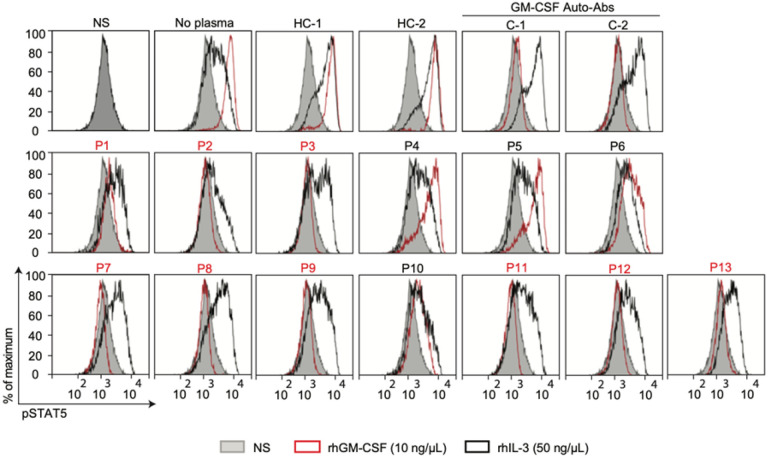 Figure 1
Figure 1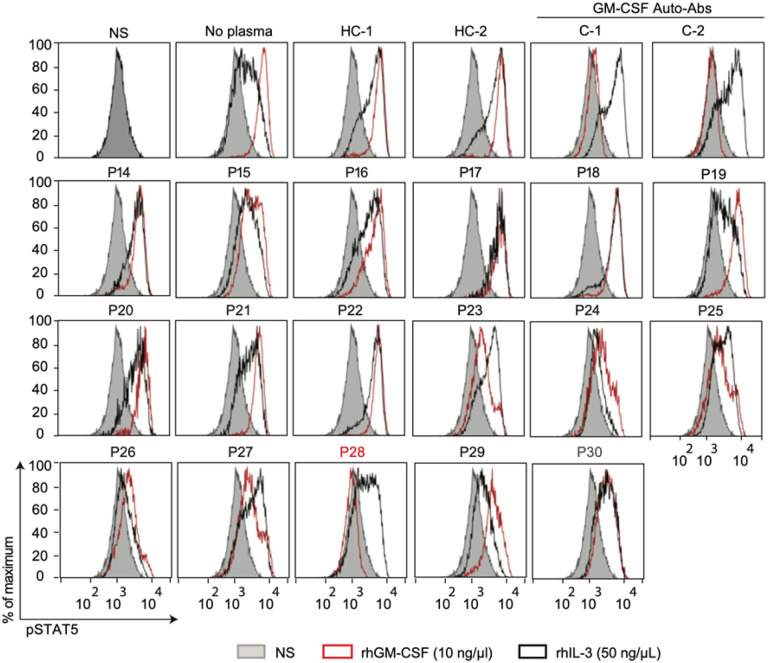 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Antifungal resistance and susceptibility · Immunodeficiency and Autoimmune Disorders
Introduction
Cryptococcosis is initiated by breathing blastoconidium or basidiospores of the yeasts of the species complexes Cryptococcus neoformans and C. gattii [1]. After inhaling the propagules from the environment, mainly soil, avian excreta, trees, and decaying wood, cryptococcal infection presents initially as pneumonia, to later disseminate to the central nervous system (CNS), causing meningitis, the most frequent form, or even meningoencephalitis [1].
Despite common environmental exposure to cryptococcal species, cryptococcosis is rare in the healthy population because of high natural resistance. Defects in T cell-mediated immunity, specifically the decline in number and function of CD4^+^ lymphocytes, which usually occurs in people infected with the human immunodeficiency virus (HIV), remains the main risk factor to acquire infection by C. neoformans [1]. Cryptococcosis caused by C. gattii, which is much less common (~ 20%), has traditionally been associated in otherwise healthy individuals, particularly HIV-seronegative, or those with unidentified risk factors [2]. However, other immunosuppressive and pulmonary diseases are underlying conditions that have been associated with a significant higher risk of C. gattii infection [2]. Moreover, in the last decade, subtle immunologic alterations, which are host-dependent risk factors, have been detected in most patients with cryptococcosis by C. gattii, placing this species as an opportunistic pathogen [3, 4].
Anti-cytokine neutralizing autoantibodies (auto-Abs) are considered to constitute autoimmune phenocopies of Inborn Error of Immunity (IEI) with selective predisposition to infectious diseases [5–7]. Indeed, by blocking the biological function of their target cytokines, these auto-Abs cause clinical phenotypes mimicking those of IEI of the corresponding cytokines or their receptors [7]. Patients affected by different infectious diseases, including fungal infections, have been found to carry such neutralizing auto-Abs [5]. For example, chronic mucocutaneous candidiasis is attributed to interleukin (IL)-17A/F auto-Abs, adult-onset susceptibility to mycobacterial disease to interferon-gamma (IFN-γ) auto-Abs, recurrent staphylococcal infection to IL-6 auto-Abs, and more recently, severe SARS-CoV2 infection to type I IFNs auto-Abs [5, 7].
Since 2013, high titers of immunoglobulin G (IgG) auto-Abs neutralizing granulocyte-macrophage colony-stimulating factor (GM-CSF) have been identified in patients with adult-onset isolated idiopathic disseminated diseases, mostly cryptococcosis, almost exclusively by C. gattii [8–10], and other infections such those caused by species of Nocardia and more rarely Aspergillus [9, 10]. In addition to the infectious phenotype, those auto-Abs against GM-CSF have also been associated with pulmonary alveolar proteinosis (PAP), a severe lung disease characterized by the accumulation of surfactant in the alveoli, with progressive respiratory failure and an increased risk of secondary infections [11]. The causality among the presence of neutralizing auto-Abs GM-CSF and these two clinical phenotypes (PAP and cryptococcosis) is not well understood. Nevertheless, patients with such auto-Abs presenting with cryptococcosis have been reported with or without PAP manifestations, and patients with PAP have been described with or without cryptococcosis [8]. Finally, the presence of auto-Abs against GM-CSF in those pathologies, suggests an important role of GM-CSF in the correct maturation and function of alveolar macrophages, which constitutes the main cellular component of immunity against Cryptococcus [12, 13].
The fact that about 13% of cases of cryptococcosis in Colombia occur in non-HIV patients with no apparent risk factor [14, 15], together with the recent identification of auto-Abs neutralizing GM-CSF in three Colombian patients with cryptococcal meningitis by Cryptococcus spp. [16], prompted us to hypothesize that other Colombian patients affected by this mycosis and who had been regarded as otherwise healthy individuals, especially given that they were not infected with HIV, have a hidden immune dysfunction. As such, the aim of this study was to establish the presence of auto-Abs against GM-CSF in plasma or serum from 30 Colombian patients, without HIV, who developed cryptococcosis by C. gattii or C. neoformans species complexes, and to correlate our findings with the patients’ clinical data.
Materials and methods
Subjects and sera selection
As part of the National Surveillance Program for Cryptococcus and cryptococcosis in Colombia, led by the Instituto Nacional de Salud, in Bogota, Colombia, 1974 surveys from patients with cryptococcosis have been filled out between 1997 and 2016. In summary, the survey contains demographic data, risk factors, clinical manifestations, diagnostic methods, and the patients’ initial treatment [14]. From these surveys, 392 (19.9%) patients were reported without evident HIV infection (HIV negative), from whom, the etiological agent causing cryptococcosis was identified in 343 cases, 292 (85.1%) caused by C. neoformans and 51 caused by C. gattii (14.9%) [14] (See supplementary Annex 1). From all non-HIV-related cryptococcosis, only 30 patients’ serum samples were collected in a 15-year period, from 1997 to 2011, and stored in the sera collection of the Microbiology Group at the Instituto Nacional de Salud. From these available samples, which were used to establish the presence of GM-CSF auto-Abs, 13 sera were from patients with cryptococcosis by C. gattii and 17 sera by C. neoformans [14] (See in supplementary Tables S1, S2 and S3).
As part of the diagnosis of cryptococcosis, which was done by direct visualization of the encapsulated blastoconidia in cerebrospinal fluid (CSF) using India ink, some of the studied sera had data on the titter of the cryptococcal antigen (CrAg) detected in this sample. CrAg titter was also established in CSF of some patients. All isolates of C. gattii or C. neoformans causing cryptococcosis in the studied patients were identified by routinely used phenotypic methods. Most C. gattii isolates had data on antifungal susceptibility testing, serotype, mating type, molecular type and sequence type (ST), while most C. neoformans isolates had only data on serotype, mating type and molecular type [14, 15, 17] (Tables S4 and S5). All studied sera had in addition total levels of IgG, IgA and IgM, as well as cryptococcal-specific IgG, IgA and IgM, as established previously [18]. For some analysis, data on specific levels of serum immunoglobulins against cryptococcal proteins were used from serum from adults without cryptococcosis or any other infectious disease (healthy controls) [18] (See in supplementary Figures S1 and S2 ).
Detection of neutralizing GM-CSF auto-Abs by flow cytometry
Human peripheral blood mononuclear cells (PBMCs) from a healthy donor were isolated from whole blood by Ficoll- Hypaque density centrifugation (Amersham-Pharmacia- Biotech). The cells were counted and plated at 2 × 10^6^ cells/well in 96-well V-bottom plates (Thermo-Fisher-Scientific), in 100 μL of RPMI (GibcoBRL, Invitrogen) supplemented with 10% fetal bovine serum (GibcoBRL, Invitrogen), or 100 μL of RPMI supplemented with 1:10 serafrom patients or controls. PBMCs were left unstimulated or were stimulated with 10 ng/μL of rhIL-3 or GM-CSF or 50 ng/μL of rhIL-3 (Miltenyi-Biotec) for 15 min at 37°C. Thereafter, cells were fixed and permeabilized with a fixation/permeabilization kit (eBioscience). Extracellular labeling was performed with antibodies anti CD14-Pacific Blue and anti CD4-FITC (Sony-Biotechnology, clones M5E2 and RPA-T4, respectively). Cell viability was determined with the Aqua Dead Cell Stain Kit (Thermo-Fisher-Scientific). STAT5 phosphorylation (p-STAT5) levels were assessed by intracellular staining with Phospho-Flow PE Mouse Anti-p-STAT5 (pY694) antibody (BD Biosciences). Data were collected with a Gallios flow cytometer (Beckman-Coulter) and analyzed with FlowJo software v.10.6.2 (Becton–Dickinson).
Statistical analysis and data availability
p-value was calculated among groups with a Chi-square test with Fisher’s correction (given the low n in some of the cells of the contingency tables). A p-value < 0.05 was considered as statistically significant. All raw and processed data will be made available by the corresponding authors upon request.
Results
Cryptococcosis in Colombian HIV negative patients
Demographic and clinical characteristics of the 30 studied patients are summarized in the supplementary material (Supplementary Tables 1, 2 and 3). From them, 21 (70%) were men and nine (30%) were women, ranging from 1 to 71 years old, with an average age of 40.8 years. While most patients (86.7%) did not have any recognizable predisposing factor, hematological malignancy was registered in two patients (6.7%) as well as systemic lupus erythematosus (SLE) and rheumatoid arthritis in one patient each (3.3%). Signs and symptoms of cryptococcosis were variable among the studied patients, however, headache (70%), mental confusion (46.7%) and nausea (40%) were the most frequent clinical manifestations, considering that most patients (96.7%) were diagnosed with cryptococcal meningitis. Treatment was mainly amphotericin B deoxycholate alone (46.7%), or in combination with fluconazole (30%). Outcome of patients was recorded in 11 cases, from whom eight recovered after treatment while three died of cryptococcosis [14]
Detection of neutralizing GM-CSF auto Abs in patients’ sera
First, we evaluated the C. gattii patient’s cohort; unlike serum from healthy individuals, serum from nine patients (69.2%), incubated with 10 ng/μL of GM-CSF prevented GM-CSF-induced p-STAT5, whereas the level of IL-3-induced p-STAT5 was similar in cells incubated with controls or patients’ sera (Fig. 1). Regarding the C. neoformans cohort, one out of 17 s patients (6%) presented neutralizing GM-CSF auto-Abs (Fig. 2). Altogether, these results strongly suggest that the presence of circulating neutralizing GM-CSF auto-Abs is the risk factor to develop cryptococcosis in 10 of the studied patients.
Clinical and immunological correlation in patients with neutralizing GM-CSF auto-Abs
From the 30 studied patients, nine (69.2%) and one (6%) patient affected with cryptococcosis by C. gattii and C. neoformans, respectively, were positive for neutralizing GM-CSF auto-Abs. The demographic, clinical and microbiological characteristics of both groups (positive and negative for neutralizing GM-CSF auto-Abs) are compared (Table 1),. Clearly, patients with neutralizing GM-CSF auto-Abs are predominantly affected by C. gattii. Sex, age, and clinical presentation did not differ among patients with and without neutralizing GM-CSF auto-Abs. Clinical characteristics of patients with cryptococcosis with and without neutralizing GM-CSF auto-Abs respectively, are summarized in Supplementary Tables 2–3. Total and specific levels of immunoglobulins were determined, however total levels of IgG, IgM and IgA did not differ between patients with or without neutralizing GM-CSF auto-Abs, nor if they were infected by C. neoformans or C. gattii (Supplementary Fig. 1a–c). When compared with healthy controls, we observed higher levels of total IgG in patients with cryptococcosis, whereas total IgA and IgM were in lower levels. Nevertheless, sera from patients with cryptococcosis by C. gattii with neutralizing GM-CSF auto-Abs showed higher levels of specific IgG against cryptococcal proteins, compared to healthy controls, as established elsewhere (Supplementary Figs. 1d–e) [18].
Phenotypic and genotypic characteristics of cryptococcal isolates do not differ among patients with and without neutralizing GM-CSF auto-Abs
All C. gattii isolates causing cryptococcosis in patients with and without neutralizing GM-CSF auto-Abs, which had data on antifungal susceptibility testing, distributed among the wild-type population of the species, per antifungal drug (Supplementary Tables 4 and 5). This means that none of them showed resistance or decreased susceptibility to any antifungal drug. In addition, C. gattii isolates recovered from patients with and without neutralizing anti GM-CSF auto-Abs, did not differ regarding the serotype, mating type, molecular type, and ST of the isolates (Supplementary Fig. 1f). Serotype, mating type and molecular type did not differ either among the C. neoformans isolates.
Discussion
Our study reports neutralizing GM-CSF auto-Abs in 10 Colombian patients who developed cryptococcosis, even though these patients were deemed as otherwise healthy, based upon their clinical history at the time of diagnosis of this mycosis [14]. We also evidence that this subtle immunologic alteration prevails in patients affected by C. gattii, compared with patients affected by C. neoformans, which adds to the differences described in the epidemiology of patients with cryptococcosis caused by one species complex or another [3, 4]. Remarkably, the risk factor of patients with C. gattii infection and 16 with C. neoformans infection, remains hidden, as neutralizing auto-Abs against GM-CSF were not detected.
The epidemiology of cryptococcosis has focused especially on patients with HIV, the major risk factor for infection [19]. Though, in recent years, different studies on cryptococcosis have drawn attention to the increase in those apparently otherwise healthy individuals without HIV infection [20–23]. In Colombia, in the cryptococcoses survey performed between 1997–2016, HIV infection was found in 75.4% of patients and non-HIV in 24.6% [14]. In Brazil, HIV infection remains the main risk factor for cryptococcosis (82–86%) [24, 25], however, in a series of 29 patients without HIV infection and who did not receive transplants, 77.8% of the patients had no apparent risk factor and the majority were infected by C. gattii [21]. Similarly, in the French Guiana, HIV infection has been reported as the main risk factor for cryptococcosis (67.4%), but it was precisely in this country where was reported the first two cases of Latin-American patients with cryptococcosis presenting anti-GM-CSF auto-Abs in otherwise healthy individuals with C. gattii infection [26].These observations indicate that the epidemiology of cryptococcosis is changing with a notable increase of non-HIV-related infection suggesting that additional risk factors may be involved in the susceptibility to cryptococcosis.
In Colombia, 1974 patients with cryptococcosis have been identified between 1997 and 2016. From them, just 392 patients were HIV-negative, of whom 51 (14.9%) were affected by C. gattii infection. The study of 13 patients with C. gattii and 17 with C. neoformans from this cohort allows us to establish that those auto-Abs collectively account for 68% (n = 9) of C. gattii patients and 6% (n = 1) of C. neoformans, showing that GM auto-Abs underlie cryptococcosis in a significant proportion of cases. Nevertheless, cryptococcosis remains unexplained in most HIV-negative patients affected with C. neoformans and one-third of C. gattii. IEI of GM-CSF pathway cytokine or their receptors might potentially explain a proportion of these remaining cases. Similarly, to previous studies, all 10 patients with GM-CSF auto-Abs described here were adults (23 to 67 years old). If those auto-Abs were present before cryptococcal infection and if they remained silent up to cryptococcal infection, remains unknown. Recent studies of auto-Abs against cytokines as a main risk factor for a specific infectious disease have demonstrated the causality of those auto-Abs [27–29]. Pre-existing Type I IFN neutralizing auto-Abs is the main clear example as a risk factor for several viral diseases such as life-threatening COVID-19 pneumonia (15–20%), a third of the rare life-threatening adverse reactions to yellow fever vaccination [28], and about 40% of cases of West Nile virus encephalitis [30]. In addition, these auto-Abs showed to be present in around ~0.3% of the general population under 65 years, whereas this prevalence increases sharply after 70 years to ~4% [28–30]. The actual prevalence of GM-CSF auto-Abs in patients with cryptococcosis or healthy populations remains elusive.
Interestingly, one patient described here (P28) presented disseminated cryptococcosis by C. neoformans and pulmonary tuberculosis (Tb) by Mycobacterium tuberculosis (Mtb) one year after the cryptococcal diagnosis. To our knowledge, this is the third adult patient with disseminated cryptococcosis and neutralizing anti-GM-CSF auto-Abs who have developed Tb [8, 16]. Furthermore, mice studies and ex vivo studies, and human monocyte-derived macrophages [31–33], and our date suggest that intact GM-CSF signaling is crucial for the appropriate alveolar macrophage functions to mediate the immunity to Cryptococcus spp., and possibly against Mtb lung infection in humans.
Our findings support the hypothesis, and the new research front, that auto-Abs against cytokines may explain the susceptibility to Cryptococcus infection in otherwise healthy HIV-negative individuals [7]. However, routinely used laboratory technologies do not detect such specific targets [16, 34, 35], and ow cytometry and particle-based technology used to screen for the presence of anti-cytokines auto-Abs, are very expensive, not often available in the clinical setting and, so far, have been utilized as research tools rather than as commonly used techniques to help establishing a definitive diagnosis in patients with Infectious diseases, like cryptococcosis [8, 9, 16, 36].
Conclusions
Our findings, therefore, support the association between neutralizing GM-CSF auto-Abs and cryptococcosis, which has been described for a decade [34–36]. These auto-Ab can be totally silent until the patients are diagnosed with cryptococcosis. However, the reason why patients with this predisposing factor are more susceptible to acquire infection by C. gattii than by C. neoformans, remains elusive. Anti-GM-CSF auto-Abs are associated with some cases of pulmonary and meningeal cryptococcosis in otherwise healthy individuals. Our data support the idea that GM-CSF is a critical actor in host defense against Cryptococcus.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kwon-Chung KJ, Cryptococcus neoformans and Cryptococcus gattii, the etiologic agents of cryptococcosis. Cold Spring Harb Perspect Med. 2014;4(7):a 019760.24985132 10.1101/cshperspect.a 019760 PMC 4066639 · doi ↗ · pubmed ↗
- 2Mac Dougall L, Risk factors for Cryptococcus gattii infection, British Columbia, Canada. Emerg Infect Dis. 2011;17(2):193–9.21291588 10.3201/eid 1702.101020 PMC 3204768 · doi ↗ · pubmed ↗
- 3Kwon-Chung KJ, Saijo T. Is J Fungi (Basel). 2015;1(2):154–67.10.3390/jof 1020154 PMC 508461727795955 · doi ↗ · pubmed ↗
- 4Chen SC, Meyer W, Sorrell TC. Cryptococcus gattii infections. Clin Microbiol Rev. 2014;27(4):980–1024.25278580 10.1128/CMR.00126-13PMC 4187630 · doi ↗ · pubmed ↗
- 5Puel A Human autoantibodies underlying infectious diseases. J Exp Med, 2022. 219(4).10.1084/jem.20211387 PMC 895268235319722 · doi ↗ · pubmed ↗
- 6Ku CL, Autoantibodies against cytokines: phenocopies of primary immunodeficiencies? Hum Genet. 2020;139(6–7):783–94.32419033 10.1007/s 00439-020-02180-0PMC 7272486 · doi ↗ · pubmed ↗
- 7Vinh DC. Of Mycelium and Men: Inherent Human Susceptibility to Fungal Diseases. Pathogens, 2023. 12(3).10.3390/pathogens 12030456 PMC 1005861536986378 · doi ↗ · pubmed ↗
- 8Rosen LB, Anti-GM-CSF autoantibodies in patients with cryptococcal meningitis. J Immunol. 2013;190(8):3959–66.23509356 10.4049/jimmunol.1202526 PMC 3675663 · doi ↗ · pubmed ↗