Implementation of a monitoring and contact tracing program to manage COVID-19 by a multinational chemical company
Daniel Astun Cirino, Henrique Ceretta Oliveira, Ariane Polidoro Dini, Marcia Bandini

TL;DR
A multinational chemical company implemented a contact tracing program to manage COVID-19, finding that age, symptoms, remote work, and emotional distress were linked to infections.
Contribution
The study demonstrates how workplace data can identify risk factors and inform health interventions during a pandemic.
Findings
1190 confirmed COVID-19 cases were identified out of 4206 reports between 2020 and 2022.
Age over 40, being symptomatic, remote work, and emotional distress were associated with infection.
On-the-job education and mental health monitoring were highlighted as important for worker protection.
Abstract
During the SARS-CoV-2 pandemic, uninterrupted manufacture of products for domestic or health care purposes presupposed initiatives to control transmission in the work environment. This study analyzed data collected in a multinational chemical company between 2020 and 2022 through its COVID-19 contact tracing system, determining the association between work variables, personal protective equipment use, emotional distress symptoms, and diagnostic confirmation of COVID-19. This correlational, cross-sectional study analyzed a company database of reports of suspected cases between June 2020 and January 2022. Descriptive analysis was performed, and the chi-square test was used to study the associations between the variables, with a significance level of 5%. Of the 4206 total reports, 1190 diagnoses of COVID-19 were confirmed. The following variables were associated with infection: age over…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
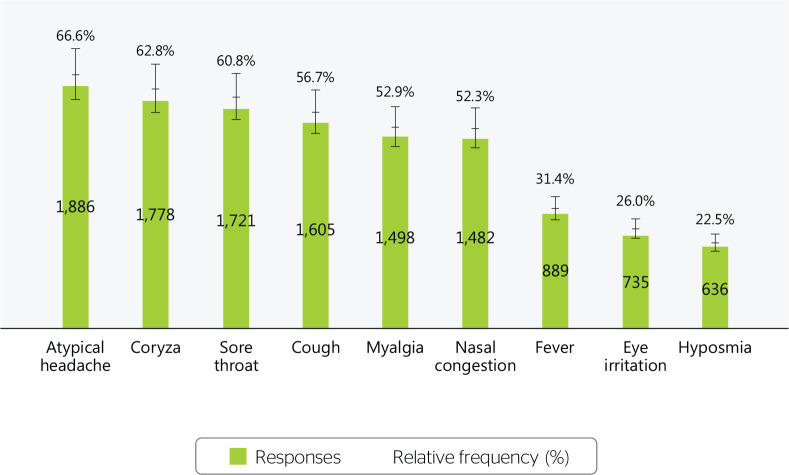 Figure 1
Figure 1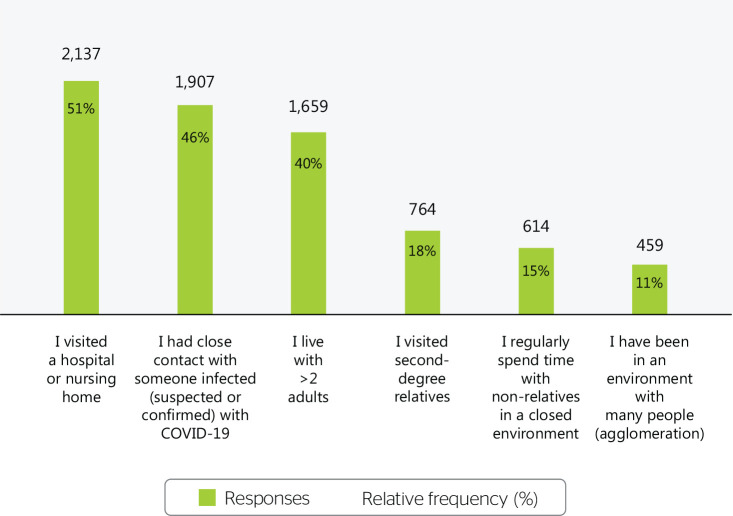 Figure 2
Figure 2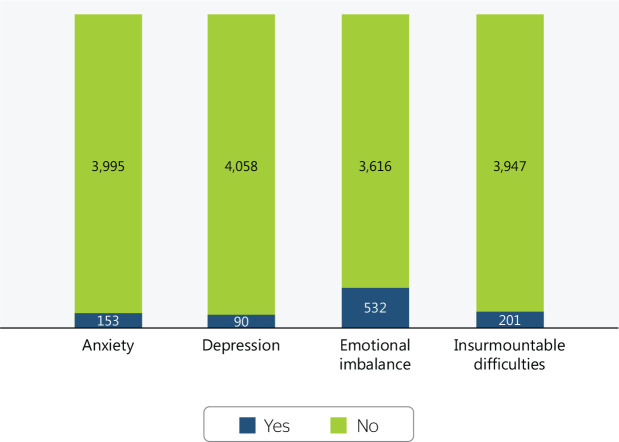 Figure 3
Figure 3| Variable | Answers | |
|---|---|---|
| n | % | |
| Age (years) | ||
| ≤ 19 | 91 | 2.2 |
| 20-29 | 1,062 | 25.2 |
| 30-39 | 1,680 | 39.9 |
| 40-49 | 1,004 | 23.9 |
| 50-59 | 317 | 7.5 |
| ≥ 60 | 8 | 0.2 |
| No data | 44 | 1.1 |
| Company branches in Brazil | ||
| Plant 1 | 1,798 | 42.8 |
| Plant 2 | 1,315 | 31.3 |
| Plant 3 | 559 | 13.3 |
| Plant 4 | 299 | 7.1 |
| Plant 5 | 212 | 5.0 |
| Plant 6 | 23 | 0.5 |
| Work shift | ||
| Morning | 1,341 | 31.9 |
| Evening | 1,075 | 25.6 |
| Night | 512 | 12.2 |
| Administrative | 1,205 | 28.6 |
| 12 x 36 | 73 | 1.7 |
| Work format during the pandemic | ||
| In person | 3,405 | 81.0 |
| Remote | 508 | 12.0 |
| Hybrid | 293 | 7.0 |
| Type of employment contract | ||
| Hourly | 2,562 | 60.9 |
| Monthly | 700 | 16.6 |
| Outsourced | 944 | 22.5 |
| Variable | Answers | |
|---|---|---|
| n | % | |
| N-compliance with preventive protocols | ||
| No | 4,139 | 98.4 |
| Yes | 67 | 1.6 |
| COVID-19 diagnosis | ||
| Negative | 3,016 | 71.7 |
| Positive | 1,190 | 28.3 |
| Close contact in the workplace | ||
| No | 3,766 | 89.5 |
| Yes | 123 | 2.9 |
| No data | 317 | 7.6 |
| Variable | COVID-19 diagnosis | p-value | |||
|---|---|---|---|---|---|
| Negative | Positive | ||||
| n | % | n | % | ||
| Age (years) | <0.0001 | ||||
| ≤29 | 887 | 76.93 | 266 | 23.07 | |
| 30-39 | 1,202 | 71.55 | 478 | 28.45 | |
| 40-49 | 672 | 66.93 | 332 | 33.07 | |
| ≥50 | 228 | 69.94 | 98 | 30.06 | |
| Work model | <0.0001 | ||||
| Remote | 276 | 54.33 | 232 | 45.67 | |
| In person/hybrid | 2,740 | 74.09 | 958 | 25.91 | |
| Type of employment contract | <0.0001 | ||||
| Hourly | 1,862 | 72.68 | 700 | 27.32 | |
| Monthly | 428 | 61.14 | 272 | 38.86 | |
| Outsourced | 726 | 76.91 | 218 | 23.09 | |
| N95 respirators used in work activity? | <0.0001 | ||||
| No | 647 | 64.00 | 364 | 36.00 | |
| Yes | 2,312 | 74.51 | 791 | 25.49 | |
| Close contact with a positive COVID-19 case in the last 2 weeks? | <0.0001 | ||||
| No | 2,400 | 73.42 | 869 | 26.58 | |
| Yes | 610 | 65.95 | 315 | 34.05 | |
| Have you had any COVID-19-related symptoms in the last 15 days? | <0.0001 | ||||
| No | 1,049 | 77.47 | 305 | 22.53 | |
| Yes | 1,965 | 69.00 | 883 | 31.00 | |
| Difficulty controlling feelings and reactions to unforeseen events? | |||||
| Never/rarely | 2,875 | 72.18 | 1,108 | 27.82 | 0.0105 |
| Frequently/always | 104 | 63.03 | 61 | 36.97 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfection Control and Ventilation · COVID-19 Pandemic Impacts · COVID-19 and Mental Health
INTRODUCTION
The COVID-19 pandemic greatly impacted the world of work through measures to control transmission, provide safety, and protect worker health. Factories adapted their production spaces and common areas, implementing new rules, procedures, control measures, and equipment usage.^1-3^
Being an infectious disease transmitted primarily through respiratory droplets during close in-person contact, preventing the transmission of COVID-19 in the workplace is largely based on the following strategies: physical distancing, constant mask usage, greater ventilation, hygienization of hands and workplaces, self-observation for signs and symptoms, identification of suspected cases for isolation and monitoring, and testing for diagnostic confirmation.^4,5^
Contact tracing/mapping was an important procedure for controlling the spread of COVID-19 since it proactively identified potentially infected individuals, whether symptomatic or asymptomatic, allowing company occupational health services to refer them for isolation or quarantine, thus combating transmission.^6,7^
The emergence of new variants of the SARS-CoV-2 virus, the occurrence of sequential epidemic outbreaks (popularly known as “new waves”) and the unequal distribution of COVID-19 vaccines, as well as raw material restrictions that resulted in production shortfalls, created a complex and challenging global scenario for satisfactory pandemic control.^1-3,5,7^
The economic and social crises surrounding the pandemic have made it difficult for companies to maintain operations, providing employment and income to workers in a context of greater volatility, uncertainty, complexity, and ambiguity (VUCA) and in the global market.^6,8,9^ The term “VUCA” was coined by the U.S. Army War College in the late 1980s in reference to post-Cold War geopolitics, and its use in the corporate environment has been renewed during extraordinary situations, such as the recent pandemic.^8,9^
The production of personal protective masks, respirators, health care materials, and household products, which are critical even for those able to remain isolated during the COVID-19 pandemic, has continued uninterrupted. However, controlling the transmission of SARS-CoV-2 in the workplace is a collective health initiative that presupposes managerial initiatives to promote health and prevent worker illness.^1,5^
This study investigated workplace epidemiological surveillance and strategies to control the spread of COVID-19, analyzing a multinational chemical industry’s contact tracing data for COVID-19 between 2020 and 2022, verifying the association between work variables, personal protective equipment use, emotional distress symptoms, and diagnostic confirmation of COVID-19 in workers.
METHODS
This quantitative, correlational, cross-sectional study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies. It was conducted in a multinational corporation that develops essential products for society and, within the scope of legislation regarding the COVID-19 pandemic, production was maintained to avoid shortages. The company’s diverse product range encompasses health care, personal protective equipment, consumer goods, food safety, and the transportation, electronics, automotive, and aerospace industries. During the pandemic, it manufactured high-performance masks for respiratory protection, known as filtering facepiece respirators. In Brazil, where the study was conducted, the company has 3,300 permanent employees and approximately 2,000 subcontracted workers.
Data was collected from a corporate occupational medicine database developed prior to the study to monitor suspected COVID-19 cases among workers. The company’s legal department authorized our use of the database for research purposes. This research project was approved the institutional research ethics committee (5,198,871). After ethical approval, the database was analyzed, excluding data that could identify individual workers. This study complied with Brazilian Resolution 466/12, which concerns research involving human beings.
The database consisted of reports of suspected cases occurring between June 2020 and January 2022, including the following variables: age, sex, symptoms, work characteristics, respirator use, potential exposure to SARS-CoV-2 in the workplace (by describing close contact with suspected cases), work model (remote, hybrid, or in-person), work shift, and confirmed COVID-19 diagnosis.
The data were exported to Microsoft Excel spreadsheets. Pearson’s Chi-square test was used to determine the associations between qualitative variables and confirmed COVID-19 diagnosis. A significance level of 5% was used for all analyses.^10^
RESULTS
The database included reports of 4206 suspected cases between June 2020 and January 2022. It should be pointed out that the database consists of responses rather than respondents, ie, one worker could have contributed multiple reports.
The most common worker age range was 30-39 years (39.9%), followed by 20-29 years (25.2%), 40-49 years (23.9%), 50-59 years (7.5%), <20 years (2.2%), and >60 years (0.2%). Regarding plant location, 92.9% of the reports were from workers in the state of São Paulo (Plants 1, 2, 3, 5 and 6) and 7.1% from the Manaus plant (Plant 4). Among the 4206 workers, the most prevalent shifts, in descending order, were: morning (31.9%), administrative (28.6%), afternoon (25.6%), night (12.2%), and 12-for-36 (ie, 12-hour workdays on alternate days) (1.7%).
The work models during the pandemic, in descending order of prevalence, were in-person (80.9%), hybrid (12.1%) and remote (7%). There were 3 employment types: hourly (61%), ie, those directly involved in industrial production; monthly (16.6%), ie, those with predominantly administrative activities; and outsourced (22.5%), ie, service providers and suppliers. There was a higher prevalence of hourly and in-person workers (Table 1).
Table 1: Distribution of sociodemographic and work-related characteristics, Brazil, 2020-2022
Regarding the tracing and monitoring of COVID-19 among workers, adherence to preventive protocols was quite high (98.4%), and there was a low frequency of risky situations, such as close contact in the work environment (2.9 %) (Table 2). Among all 1190 responses during the study period, 28.3% corresponded to workers who tested positive for COVID-19.
The main symptoms mentioned in the contact tracing interview were headache (66.6%), runny nose (62.8%), sore throat (60.8%), cough (56.7%), body pain (52.9%), nasal congestion (52.3%), fever (31.4%), eye irritation (26%), and reduced sense of smell or taste (22.5%) (Figure 1).
Figure 1. Main symptoms reported in contact tracing, Brazil, 2020-2022.
The main community risk situations for COVID-19 infection were: visiting a hospital or nursing home (51.6%), close contact with a sick person (46%), living with >2 adults (40%), visiting second-degree relatives (18.4%), regularly spending time with non-relatives in a closed environment (14.8%), and being in a crowd (11.1%) (Figure 2).
Figure 2COVID-19 exposure risk outside the work environment, Brazil, 2020-2022.
Regarding self-perceived emotional state, 12.8% (n = 532) reported some difficulty controlling their feelings due to unforeseen events in everyday life and 4.8% (n = 201) reported feeling that their difficulties were becoming insurmountable (Figure 3).
Figure 3. Worker self-perceived emotional state, Brazil, 2020-2022.
Workers aged < 30 years were the least infected group, while those aged > 40 years had the highest proportion of diagnosed COVID-19 cases. There was a higher proportion of COVID-19 infection among remote workers than in-person or hybrid workers. Use of a filtering facepiece respirator while working had a protective effect, ie, those who used one had a lower chance of COVID-19 infection. Symptomatic workers who had contact with someone with a diagnosed COVID-19 infection had a higher infection rate than symptomatic workers who did not and a higher infection rate than asymptomatic workers. Workers who reported difficulties controlling their feelings and reactions to unforeseen events had a higher proportion of COVID-19 infection than those who did not report such difficulties (Table 3).
DISCUSSION
Workers who participated in the contact tracing process were predominantly between 30 and 39 years of age (40% of the overall reports; 28% of the confirmed COVID-19 cases), although there was a higher proportion of cases among workers aged 40-49 years (24% of the overall reports; 33% of the confirmed COVID-19 cases).
According to chronic non-communicable disease prevalence data, systemic arterial hypertension and diabetes mellitus occur 18% and 4% of Brazilians aged 35 to 44 years, respectively, and in 34% and 8% of those aged 45 to 54 years, respectively.^11^ Considering that COVID-19 can increase the risk of worsening comorbidities,^11,12^ in addition to the cardiovascular clinical repercussions of long COVID-19, suspected case monitoring and contact tracing programs must pay special attention to workers aged 40 to 49 years.
Regarding work characteristics, 88% of the reports were from in-person or hybrid model workers (≥2 days of in-person work per week) workers, ie, the bulk of those who used company facilities and were subject to monitoring, given that the plants were considered high-risk locations for SARS-CoV-2 outbreaks and subsequent community transmission.^13^ Another important fact is that 22% of the population was outsourced workers (service providers), which indicates that all workers who operated in the same work environment were included without distinction according to employment relationship, revealing the thorough level of support and epidemiological coverage.^13^
Regarding adherence to preventive protocols, 123 potential exposure events were reported in the work environment, as opposed to 1907 such events outside the work environment, the majority of which involved health care-related exposure (51% in visits to hospitals or nursing homes), housing (living with >2 adults in the same house), and family visits.
The interesting results for self-perceived emotional state (>95% reported no emotional distress; see Figure 3) may have been due to the following factors, which could positively affect mental health: the availability of personal protective equipment, training, a positive work environment (trust), and emotional support.^14,15^
There was a positive association between lower relative frequency of COVID-19 diagnosis (25%) and mandatory use of filtering facepiece respirators as personal protective equipment compared to work activities for which their use was merely recommended (36%). This result corroborates the efficiency of high-performance respirators for controlling transmission, as previously demonstrated by the U.S. Centers for Disease Control and Prevention.^16^
The results suggest that in-person work is safer than remote work (26% vs 46% of the infections), which indicates how the work environment can positively affect adherence to preventive protocols through collective control and prevention measures (such as ventilated spaces and physical distancing). The results also demonstrate the need for greater support for remote workers, as well as the effects of pandemic fatigue, which contributes to flexible behavior regarding infection risk.^17^
The contact tracing program involved identifying, minimizing, and monitoring contact with suspected and/or confirmed cases of COVID-19.^5,18^ Active searching was selected to facilitate adherence to this process, thus epidemiological surveillance was an important instrument for increasing communication and promoting initiatives to preserve and improve organizational performance.
In the context of worker health management, considering that quarantining millions of people simultaneously with no foreseeable end in sight had never been done before, the surveillance process included questions on emotional well-being to monitor negative aspects of mental health.^19^ Although the reported symptoms of mental suffering were not overly worrying, it is important to point out that data collection was not anonymous for these questions and, thus, social desirability bias must be considered, ie, respondents may have downplayed mental health symptoms.^20^ Therefore, ways to increase our understanding of the true psychological impact of the pandemic warrant further consideration.^19^
Study limitations included the cross-sectional design, which cannot identify cause and effect, as well as the fact that the first author is a medical manager at the data collection site. Regarding the potential for future research, analyzing the work environment as a protective factor for worker health is clearly relevant.
CONCLUSIONS
A data collection process was implemented for contact tracing that transcended the context of the pandemic, covering topics such as mental health and the safety of the work environment. This data provided a basis for initiatives to promote health in the workplace. According to the results, there was a lower percentage of confirmed COVID-19 infection among in-person workers than remote workers. This indicates the potential of educational activities for in-person work, as well as that of safety measures, such as high-performance respiratory protective equipment, given that modifying the work environment through control and prevention measures protected worker health. However, the results also indicated opportunities for training among remote workers.
The mental health results were inconclusive and indicate the need for professional monitoring to identify potential mental health problems and suffering due to the pandemic.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Koh D Goh HP. Occupational health responses to COVID-19: what lessons can we learn from SARS?J Occup Health 2020621 e 121283251588210.1002/1348-9585.12128 PMC 7221300 · doi ↗ · pubmed ↗
- 2Cucinotta D Vanelli M. WHO declares COVID-19 a pandemic Acta Biomed 20209111571603219167510.23750/abm.v 91i 1.9397 PMC 7569573 · doi ↗ · pubmed ↗
- 3Zhu N Zhang D Wang W Li X Yang B Song J A novel coronavirus from patients with pneumonia in China, 2019 N Engl J Med 202038287277333197894510.1056/NEJ Moa 2001017 PMC 7092803 · doi ↗ · pubmed ↗
- 4Aquino EML Silveira IH Pescarini JM Aquino R Souza-Filho JA Rocha AS Social distancing measures to control the COVID-19 pandemic: potential impacts and challenges in Brazil Cien Saude Colet 202025 suppl 1242324463252028710.1590/1413-81232020256.1.10502020 · doi ↗ · pubmed ↗
- 5Kniffin KM Narayanan J Anseel F Antonakis J Ashford SP Bakker AB COVID-19 and the workplace: implications, issues, and insights for future research and action Am Psychol 202176163773277253710.1037/amp 0000716 · doi ↗ · pubmed ↗
- 6Calvo RA Deterding S Ryan RM. Health surveillance during covid-19 pandemic BMJ 2020369 m 13733225318010.1136/bmj.m 1373 · doi ↗ · pubmed ↗
- 7Dehghani F Omidi F Yousefinejad S Taheri E. The hierarchy of preventive measures to protect workers against the COVID-19 pandemic: a review Work 20206747717773333739910.3233/WOR-203330 · doi ↗ · pubmed ↗
- 8Bennett N Lemoine GJ. What a difference a word makes: understanding threats to performance in a VUCA world Bus Horiz 2014573311317