Harmonizing Dentofacial Balance: A Comprehensive Exploration of Class 1 Malocclusion Resolution With Impacted Maxillary Central Incisor Management
Nishu Agarwal, Pallavi Daigavane, Ranjit Kamble, Dhwani Suchak, Mrudula Shinde

TL;DR
This case report explores the treatment of a rare dental issue involving an impacted tooth and its impact on facial aesthetics.
Contribution
The paper presents a case study highlighting a combined orthodontic and surgical approach for managing impacted teeth.
Findings
A 16-year-old male patient had an impacted maxillary right central incisor and a supernumerary tooth.
A combined orthodontic and surgical treatment approach was necessary for successful resolution.
The case emphasizes the challenges and solutions in treating rare dental malocclusions.
Abstract
Permanent maxillary central incisor impaction is generally a rare phenomenon. Because the anterior teeth have a huge impact on a patient's facial aesthetics, missing anterior teeth are of major concern to patients who seek orthodontic treatment. However, correcting this type of malocclusion poses a challenge to the orthodontist. This case report of a 16-year-old male patient with an impacted maxillary right central incisor takes us through a series of events that are necessary to treat this type of malocclusion. The presenting case also had an impacted supernumerary tooth which was the primary cause for permanent tooth impaction. A combined treatment approach is usually needed to manage this type of case involving both the orthodontist and the surgeon.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
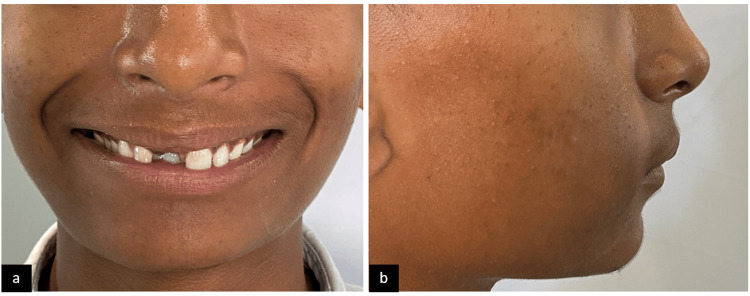 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3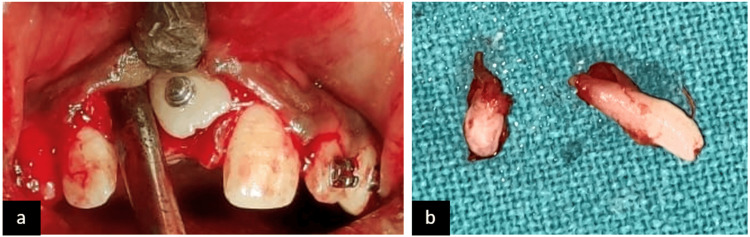 Figure 4
Figure 4 Figure 5
Figure 5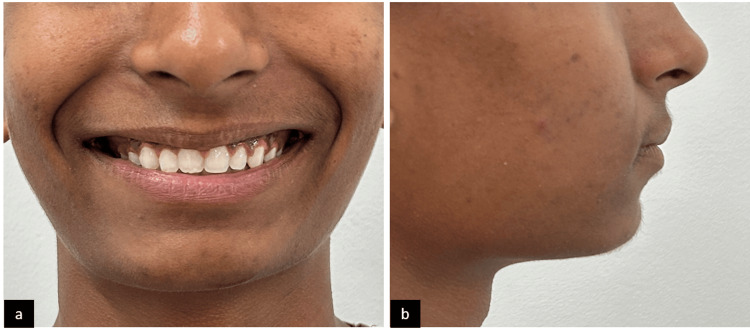 Figure 6
Figure 6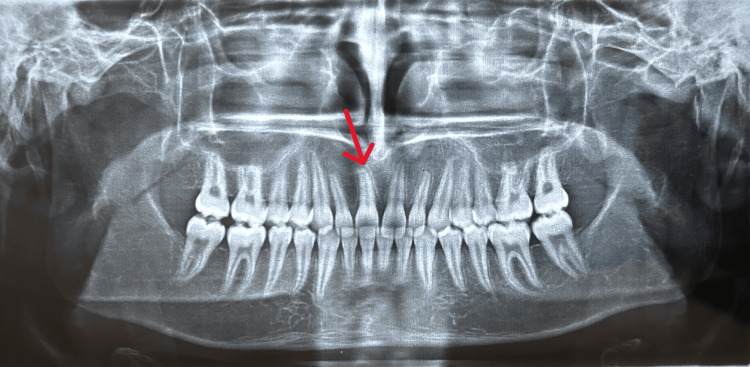 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
Topicsdental development and anomalies · Oral and Maxillofacial Pathology · Cleft Lip and Palate Research
Introduction
The main aim of orthodontic treatment focuses on achieving a healthy periodontium and a balanced functional occlusion which results in improved facial aesthetics and overall appearance of the patient. Surgical intervention is needed in cases where a permanent tooth fails to erupt in the oral cavity. Various factors associated with this impaction are thick mucosa covering the tooth, association of a cyst, supernumerary tooth associated with the impacted permanent tooth, and no space availability due to crowding in the dental arch [1].
Eruption of a tooth into the oral cavity occurs when two-thirds of the root formation is completed. If a tooth does not erupt in the age range where it should erupt, it is considered to be impacted. Surgical intervention and orthodontic treatment are usually necessary to bring the teeth into their normal alignment in the dental arch [2].
Prevalence of impaction of the maxillary central incisor is found to be 0.03-0.20%. Though this is a rare occurrence, it has a huge impact on a patient's facial aesthetics, speech, and psychology [3]. When the tooth is covered by a thick mucosa that is hindering its eruption, surgical exposure only will allow the tooth to erupt on its own, provided there is space in the dental arch. However, when other conditions as mentioned above are involved, a combination of surgical intervention and orthodontic therapy is needed to achieve the desired result [4]. If favorable conditions are not present for the eruption of the impacted tooth, other treatment options include prosthetic rehabilitation depending on the patient's case. In these cases, interdisciplinary management is needed [5].
Case presentation
The presented case is of a 16-year-old male patient with a main complaint of missing upper front teeth. No significant medical history was present. The patient had an orthognathic facial profile (Figure 1). Upon clinical examination, molars were in class 1 relationship with missing 11 (Figure 2). A panoramic radiograph was taken to assess the position and prognosis of the impacted maxillary central incisor (Figure 3).
Pre-treatment extraoral photographs: (a) frontal smiling and (b) profile
Pre-treatment intraoral photographs: (a) maxillary arch, (b) mandibular arch, (c) right molars in occlusion, (d) left molars in occlusion, and (e) anteriors in occlusion
Pre-treatment panoramic radiograph
After assessment of the case, an association of two supernumerary teeth was found with 11, and formulation of a treatment plan was done which included extraction of the supernumerary tooth and surgical exposure of the impacted tooth (Figure 4). The amount of space available in the dental arch was similar to that of the impacted tooth, i.e., 8 mm.
Surgical procedure: (a) surgical exposure of the impacted tooth and (b) extracted two supernumerary teeth
Bonding of both the maxillary and the mandibular arch was carried out. Initial leveling and alignment were done using nickel-titanium (NiTi) wires. Surgical exposure was carried out with 11, and extraction of the supernumerary tooth was done. A traction force was applied to the impacted tooth with a lingual button which was bonded onto the labial surface for forced eruption into the dental arch. After the tooth was visible in the oral cavity, a piggyback wiring was given along with a 17x25" NiTi wire to align the tooth. The treatment took about 13 months to complete, and the patient showed satisfaction with the result (Figure 5 and Figure 6). Post-treatment panoramic radiograph showed adequate bone support to the tooth (Figure 7).
Post-treatment intraoral photographs: (a) maxillary arch, (b) mandibular arch, (c) right molars in occlusion, (d) left molars in occlusion, and (e) anteriors in occlusion
Post-treatment extraoral photographs: (a) frontal smiling and (b) profile
Post-treatment panoramic radiograph
Discussion
Unerupted teeth in the anterior region can have a psychological impact on the patients. The type of treatment for these types of cases is important. Extraction of a tooth may lead to loss of the surrounding alveolar bone, so if preservation of the tooth is possible, the clinician should attempt it. The goal of an orthodontist is to preserve and align the impacted tooth, if possible, to maintain occlusal harmony and improve patients' facial aesthetics, reducing its adverse effects on patients' psychology [1].
Several factors are to be considered if there is the presence of an impacted tooth: dilaceration of the root if realignment is possible in the available space and direction, transposition, and angulation of the tooth. The extent of dilaceration, the formation of the root, and the tooth position all influence the rate of success of the impacted dilacerated tooth. If a dilacerated tooth is placed at a lower position with an obtuse angle and root formation is not complete, it will have a better prognosis for orthodontic traction [6]. The cause of dilaceration that usually leads to impaction is due to trauma during the deciduous dentition period [7].
In cases of tooth transposition, it might be difficult to treat because of the less width of the buccolingual bone. These types of cases are usually associated with trauma [8]. Many patients opt for a prosthetic replacement for the impacted tooth rather than undergoing surgical exposure. In these cases, the combined treatment plan should be formulated by both the orthodontist and the prosthodontist to improve patients' facial appearance [9,10]. In a study conducted by Khera et al., a closed eruption technique for surgical exposure was used [11]. Becker in his study concluded that the closed eruption of impacted teeth gave better results [12]. Nisa et al. [13] in their study after exposure to the impacted tooth used traction force for the eruption similar to this case. In the presented case report, the availability of space was enough to bring the impacted tooth into normal alignment; hence, no extractions were carried out and alignment of the tooth was achieved.
Conclusions
Impacted central incisor is a rare occurrence, but addressing it is of immense importance. Treatment method and treatment time depend upon the location of the tooth and various other factors discussed above. Early intervention is necessary to treat this type of malocclusion.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A case of impacted maxillary central incisor and its management J Pharm Bioallied Sci Kannan PK Palanisamy SK Kumar TS 064201210.4103/0975-7406.100263 PMC 346790223066245 · doi ↗ · pubmed ↗
- 2The unerupted maxillary central incisor: review of its etiology and treatment ASDC J Dent Child Brin I Zilberman Y Azaz B 352356491982 https://pubmed.ncbi.nlm.nih.gov/6957426/6957426 · pubmed ↗
- 3Treatment of impacted maxillary central incisors as a consequence of trauma AJO-DO Clin Companion Araujo E Tanaka OM 36738832023
- 4Management of impacted maxillary central incisor: modified Nance arch application J Contemp Dent Pract Mannathoko-Molefhe B Hu R 4154211620152616226310.5005/jp-journals-10024-1699 · doi ↗ · pubmed ↗
- 5Impacted maxillary central incisor: surgical exposure and orthodontic treatment Am J Orthod Dentofacial Orthop Pinho T Neves M Alves C 25626514020112180326410.1016/j.ajodo.2009.11.018 · doi ↗ · pubmed ↗
- 6Treatment of an impacted dilacerated maxillary central incisor Am J Orthod Dentofacial Orthop Lin YT 40640911519991019428510.1016/s 0889-5406(99)70260-x · doi ↗ · pubmed ↗
- 7Orthodontic movement of dilacerated maxillary central incisor. Report of a case Am J Orthod Kolokithas G Karakasis D 31031576197929027610.1016/0002-9416(79)90027-7 · doi ↗ · pubmed ↗
- 8Incomplete canine transposition and maxillary central incisor impaction--a case report Am J Orthod Dentofacial Orthop Wasserstein A Tzur B Brezniak N 6356391111997919959410.1016/s 0889-5406(97)70315-9 · doi ↗ · pubmed ↗