Appetite and its Regulation: Are there Palatable Interventions for Heart Failure?
Matthew M. Y. Lee, Michael E. J. Lean, Naveed Sattar, Mark C. Petrie

TL;DR
This paper explores how managing appetite and weight through diet, medications, or surgery can help treat heart failure, with promising results from new drugs like glucagon-like peptide-1 receptor agonists.
Contribution
The paper highlights the potential of appetite-regulating medications, particularly glucagon-like peptide-1 receptor agonists, in managing heart failure through weight loss.
Findings
Glucagon-like peptide-1 receptor agonists can significantly reduce appetite and achieve substantial weight loss.
The STEP-HFpEF trial showed meaningful improvements in health status for heart failure patients.
Weight loss interventions may complement existing heart failure treatments.
Abstract
Obesity is a major driver of heart failure (HF) incidence, and aggravates its pathophysiology. We summarized key reported and ongoing randomized clinical trials of appetite regulation and/or dietary energy restriction in individuals with HF. Weight loss can be achieved by structured supervised diet programs with behavioural change, medications, or surgery. The new glucagon-like peptide-1 receptor agonists alone or in combination with other agents (e.g., glucose-dependent insulinotropic polypeptide and glucagon receptor agonists or amylin analogues) potently and sustainably reduce appetite, and, taken together with dietary advice, can produce substantial, life-changing, weight loss approaching that achieved by surgery. To date, data from the STEP-HFpEF trial show meaningful improvements in health status (Kansas City Cardiomyopathy Questionnaire). Effective weight management could…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
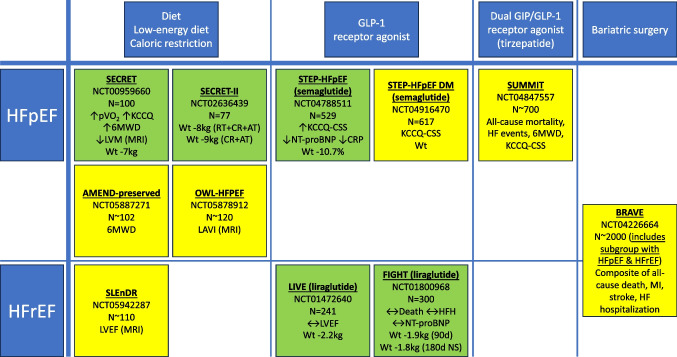 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiet and metabolism studies · Adipose Tissue and Metabolism · Cardiovascular Function and Risk Factors
Obesity and Heart Failure (HF)
Obesity increases metabolic rate and demand on the cardiovascular and respiratory systems, is a major driver of HF incidence, and aggravates its pathophysiology: the heart, like any machine, will fail if the systemic demand or load is too great. Combined, HF and obesity cause an especially poor quality of life, with more HF hospitalizations and cardiovascular deaths [1, 2].
Appetite Regulation
Appetite, defined as a desire for food, is regulated centrally by the hypothalamus, and by several hormones secreted peripherally, some in response to dietary intake.
Weight Loss
While unintentional weight loss usually indicates disease and poor prognosis, modifying appetite to induce negative caloric (energy) balance generates intentional weight loss, appears to be an efficacious treatment option for people with HF and obesity, to treat or alleviate HF and comorbidities [3–5]. Weight loss is possible with structured supervised diet programs with behavioural change, but only sustainable if appetite can be overcome or altered, by professional and lay support, changes in food choices, medications, or surgery [6]. Whilst bariatric surgery usually generates major weight loss, it is a more challenging option in the presence of HF, and late weight regain and side-effects (e.g. dumping syndrome, vitamin and mineral deficiencies, need for re-operation or reversal) are common problems. Evidence-based diet programmes including nutritional formula ‘total diet replacement’ for the weight loss phase can reliably produce weight loss > 10 kg at 12 months [6]. The new GLP-1 receptor agonists, GIP and glucagon receptor agonists, potently and sustainably reduce appetite, and, taken together with dietary advice, can produce substantial, life-changing, weight loss approaching that achieved by surgery [7, 8]. Are these strategies ‘palatable’ to individuals with HF and to healthcare systems? We recently suggested targeting more conditions earlier with weight loss may reap multiple gains (including reducing multimorbidity) beyond currently recommended treatment options [3].
Reported and Ongoing Clinical Trials (Fig. 1)
In HF with preserved ejection fraction (HFpEF), the largest diet-driven randomised trial (SECRET; n = 100) of a dietary intervention (caloric restriction (provision of all foods in a university setting)) resulted in 7 kg weight loss and improved 6-min walk distance, peak oxygen uptake, health status, and regression in left ventricular mass, compared to those who did not undergo the diet intervention [4]. Based on this one trial, caloric restriction is listed as a treatment option in international guidelines and expert consensus documents [9, 10]. Other diet trials in HFpEF were smaller, non-randomised, or achieved only modest weight loss (< 10 kg) [11, 12]. In STEP-HFpEF (n = 529) the GLP-1 receptor agonist semaglutide reduced weight by 10.7 %, improved health status, reduced a hierarchical composite endpoint, improved exercise function, and reduced inflammation and NT-proBNP [5]. In HF with reduced ejection fraction (HFrEF), dietary studies have been small or non-randomised [13]. In HFrEF, two trials in non-obese populations of the GLP-1 receptor agonist liraglutide achieved trivial weight loss (~ 2 kg); there were very small numbers of clinical endpoints in these trials, rendering unclear conclusions [14, 15]. There are no randomized trials of bariatric surgery in HFpEF or HFrEF, only observational evidence that supports a potential benefit from intentional weight loss [16]. The ongoing BRAVE open-label randomized controlled trial (NCT04226664) is assessing bariatric surgery versus medical weight management and will recruit ~ 2000 patients with high-risk cardiovascular disease (including, importantly, a subgroup (interim data n = 17/49 (35%)) with symptomatic HF) [17] (Fig. 1).Fig. 1. Key randomized trials of appetite regulation in HF (key outcomes; green = completed; yellow = ongoing; between-group differences shown except for SECRET-II where within-group differences shown). Abbreviations: 6MWD, 6-min walk distance; AT, aerobic exercise training; CR, caloric restriction; CRP, C-reactive protein; GIP, glucose-dependent insulinotropic polypeptide; GLP-1, glucagon-like peptide-1; HF, heart failure; HFH, heart failure hospitalization; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; KCCQ-CSS, Kansas City Cardiomyopathy Questionnaire Clinical Summary Score; LAVI, left atrial volume index; LVEF, left ventricular ejection fraction; LVM, left ventricular mass; MRI, magnetic resonance imaging; NS, not significant; NT-proBNP, N-terminal pro-B-type natriuretic peptide; pVO_2_, peak oxygen uptake; RT, resistance training; wt, body weight
Future Directions
From first principles, earlier, effective weight management with substantial weight loss should relieve several drivers of HF, to complement the existing treatments for HFrEF and potentially provide a vital effective intervention for HFpEF. Adequately powered outcome trials are needed to provide definitive evidence, to understand the effect of intentional weight loss on clinical events, and mechanisms of benefit. The value of combining therapies must be assessed: GLP-1/GIP/glucagon receptor agonists appear promising adjunctive treatments that warrant definitive trials, and it remains possible that some effects of these medications may be independent of weight loss. Challenges include long-term weight-loss maintenance, programme accessibility, flexibility and adherence, and costs. Hippocrates reminded us: “If we could give every individual the right amount of nourishment and exercise, not too little and not too much, we would have found the safest way to health.” [18] Healthcare systems need to target weight loss much more actively for societal and patient gains [3].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Reddy YNV Rikhi A Obokata M Quality of life in heart failure with preserved ejection fraction: importance of obesity, functional capacity, and physical inactivity Eur J Heart Fail 20202261009101810.1002/ejhf.178832150314 · doi ↗ · pubmed ↗
- 2Butt JH Petrie MC Jhund PS Anthropometric measures and adverse outcomes in heart failure with reduced ejection fraction: revisiting the obesity paradox Eur Heart J 202344131136115310.1093/eurheartj/ehad 08336944496 PMC 10111968 · doi ↗ · pubmed ↗
- 3Sattar N Mc Murray JJV Mc Innes IB Aroda VR Lean MEJ Treating chronic diseases without tackling excess adiposity promotes multimorbidity Lancet Diabetes Endocrinol 2023111586210.1016/S 2213-8587(22)00317-536460014 · doi ↗ · pubmed ↗
- 4Kitzman DW Brubaker P Morgan T Effect of caloric restriction or aerobic exercise training on peak oxygen consumption and quality of life in obese older patients with heart failure with preserved ejection fraction: a randomized clinical trial JAMA 20163151364610.1001/jama.2015.1734626746456 PMC 4787295 · doi ↗ · pubmed ↗
- 5Kosiborod MN Abildstrøm SZ Borlaug BA Semaglutide in patients with heart failure with preserved ejection fraction and obesity N Engl J Med 2023389121069108410.1056/NEJ Moa 230696337622681 · doi ↗ · pubmed ↗
- 6Lean MEJ Leslie WS Barnes AC Primary care-led weight management for remission of type 2 diabetes (Di RECT): an open-label, cluster-randomised trial Lancet 20183911012054155110.1016/S 0140-6736(17)33102-129221645 · doi ↗ · pubmed ↗
- 7Wilding JPH Batterham RL Calanna S Once-weekly semaglutide in adults with overweight or obesity N Engl J Med 202138411989100210.1056/NEJ Moa 203218333567185 · doi ↗ · pubmed ↗
- 8Jastreboff AM Aronne LJ Ahmad NN Tirzepatide once weekly for the treatment of obesity N Engl J Med 2022387320521610.1056/NEJ Moa 220603835658024 · doi ↗ · pubmed ↗