Letter to the editor: “Eliciting national and subnational sets of disability weights in mainland China: findings from the Chinese disability weight measurement study”
Thomas Hampton, Kathryn A. Haigh, Mphatso Dennis Phiri, Ewan Tomeny

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
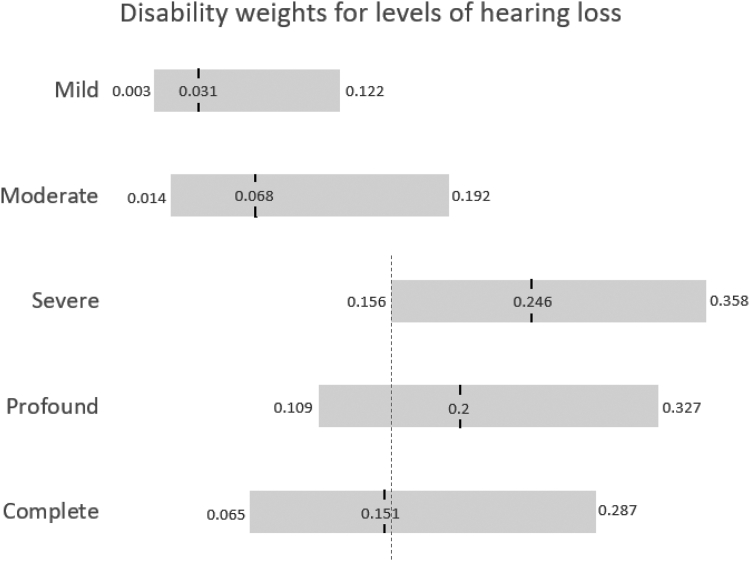 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCultural Identity and Heritage · Aging, Elder Care, and Social Issues · Contemporary art, education, critique
We commend Liu et al. for providing new disability weights (DW) based on 468,541 respondents from across mainland China following Global Burden of Disease (GBD) study methodology.1 A low proportion of respondents from China contributed to prior GBD surveys and similar studies from Japan found differences compared to the GBD DW values.2 However, some reported weights seem to defy condition severity classifications, contradicting conventional clinical and health economic expectations.
For the five ordinal states reflecting severity of hearing loss (HL), despite a clear worsening of lay descriptions, state values provided imply a benefit to complete HL over profound or severe HL (Table 1; Fig. 1). Furthermore, the weights for Tuberculosis (TB) suggest a lower disability level for individuals with TB who are additionally living with HIV. While arguments could be invoked for valid differences in care/experiences in these groups such as adjustment in social or occupational contexts, signposting, care delivery models, follow-up frequency etc,3 this cannot explain these incongruous DWs, due to worsening lay descriptions used in the weight elicitation. These DW were established by presenting participants with a selection of lay descriptions (not the whole batch or the disease state names), in a process of pairwise comparison. Health states themselves were not given, and ultimate weights were estimated using statistical modelling.1Table 1DW from Table 2 in Liu et al.1 (The DW is measured on a scale from 0 to 1, with a score of 0 indicating a state equivalent to full health and score of 1, essentially a state equivalent to death).Disability weight (95% UI)Lay descriptionsTuberculosis 16Not HIV infected0.375 (0.319–0.435)has a persistent cough and fever, is short of breath, feels weak, and has lost a lot of weight. 17HIV infected0.297 (0.216–0.390)has a persistent cough and fever, shortness of breath, night sweats, weakness and fatigue and severe weight loss.Hearing loss 105Mild0.031 (0.003–0.122)has great difficulty hearing and understanding another person talking in a noisy place (for example, on an urban street). 106Moderate0.068 (0.014–0.192)is unable to hear and understand another person talking in a noisy place (for example, on an urban street), and has difficulty hearing another person talking even in a quiet place or on the phone. 107Severe0.246 (0.156–0.358)is unable to hear and understand another person talking, even in a quiet place, and unable to take part in a phone conversation. Difficulties with communicating and relating to others cause emotional impact at times (for example worry or depression). 108Profound0.200 (0.109–0.327)is unable to hear and understand another person talking, even in a quiet place, is unable to take part in a phone conversation, and has great difficulty hearing anything in any other situation. Difficulties with communicating and relating to others often cause worry, depression, and loneliness. 109Complete0.151 (0.065–0.287)cannot hear at all in any situation, including even the loudest sounds, and cannot communicate verbally or use a phone. Difficulties with communicating and relating to others often cause worry, depression or loneliness.Fig. 1DW point estimates from Table 2 in Liu et al.1 (There is considerable overlap in 95% uncertainty intervals which could yet contain the true estimate but the DW point estimates themselves suggest a clear improvement in health state despite lay descriptions worsening [in particular, DW estimates for profound and complete HL suggest lower severity compared to the severe HL state (blue dashed line indicates lower bound of severe HL)].
From a health economic or policy position, these values are concerning, potentially leading to inappropriate conclusions. While weights are presented with uncertainty intervals, researchers often rely on point estimates. These DW values imply there would be no benefit in restoring the hearing of people with complete HL to that of an individual with severe HL (even if this could be achieved at no cost). Models using these weights could concerningly conclude that to reduce disability in a given population, an appropriate intervention might be to remove remaining hearing from some members or, for TB, suggest that coinfection with HIV is beneficial.
Others have previously expressed wider concerns regarding GBD weight derivation methodology4 and these contradictory findings may affect confidence in values assigned to other conditions, particularly across health states less easily verified than those above with well-defined severity levels. It seems necessary that future weight derivation studies sense-check for such reversals with participants, the public and/or clinicians, and we caution against the publication of weight tables containing incongruous results. These findings again raise the inherent issues that arise from using simple sentences as surrogates for complex conditions and applying a single set of DW across diverse global populations.5 Specifically, these verifiable concerns require addressing or risk worsening of health equity for populations with these conditions.
Contributors
ET and TH conceptualised the article. TH wrote the original draft of the article. ET, MDP and KAH provided additional original writing. All authors contributed equally to critical appraisal, review & editing. All authors approved final submitted version.
Declaration of interests
TH and KAH are supported by a Wellcome Trust Fellowship (203919/Z/16/Z). MDP is supported by a UK FCDO grant, OJEU reference number: 2018/S 196-44348. ET is supported by an institutional grant from UK aid: LIGHT consortium. No authors have any other potential or actual competing interests, financial or otherwise.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liu X.Wang F.Yu C.Eliciting national and subnational sets of disability weights in mainland China: findings from the Chinese disability weight measurement study Lancet Reg Health West Pac 26202210052010.1016/j.lanwpc.2022.100520 PMC 933537335910433 · doi ↗ · pubmed ↗
- 2Nomura S.Yamamoto Y.Yoneoka D.How do Japanese rate the severity of different diseases and injuries?-an assessment of disability weights for 231 health states by 37,318 Japanese respondents Popul Health Metr 1912021213389274210.1186/s 12963-021-00253-4PMC 8063365 · doi ↗ · pubmed ↗
- 3Seguiti C.Salvo P.F.Di Stasio E.Health-related quality of life (HR Qo L) from HIV patients' perspective: comparison of patient-reported outcome (PRO) measures among people living with hiv (PLWH) and other chronic clinical conditions J Patient Rep Outcomes 612022273534747610.1186/s 41687-022-00423-4PMC 8960483 · doi ↗ · pubmed ↗
- 4Charalampous P.Polinder S.Wothge J.A systematic literature review of disability weights measurement studies: evolution of methodological choices Arch Public Health 802022913533132510.1186/s 13690-022-00860-z PMC 8944058 · doi ↗ · pubmed ↗
- 5He Q.Zhou M.Yin P.Can global or national disability weights represent provincial level?BMC Publ Health 231202346110.1186/s 12889-022-14347-7PMC 999953736899365 · doi ↗ · pubmed ↗