Endoscopic management of a chronic anastomotic leak after a Billroth II procedure
Reid D. Wasserman, William F. Abel, Arnold Salzberg, Vivek Kesar, Paul Yeaton, Varun Kesar

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1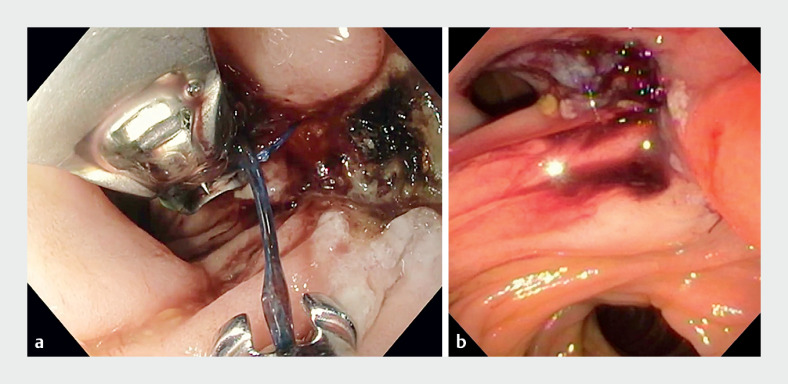 Fig. 2
Fig. 2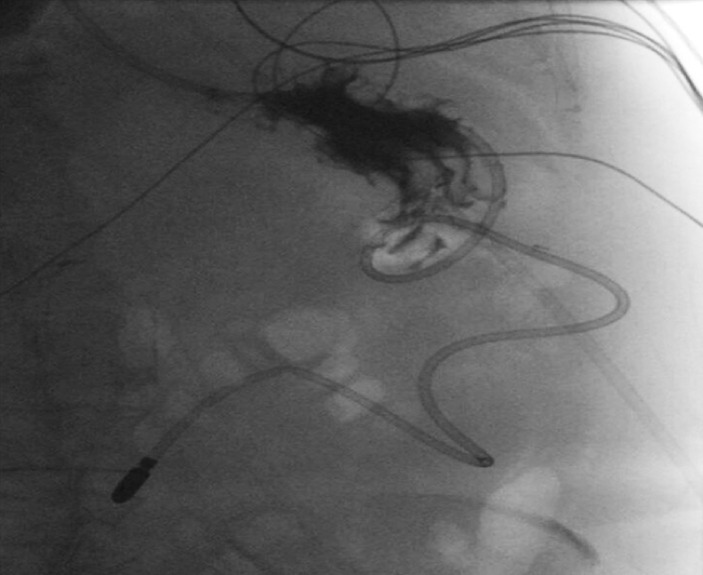 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Biliary and Gastrointestinal Fistulas · Tracheal and airway disorders
We report the case of a 56-year-old woman with a pertinent past medical history of chronic pancreatitis and peptic ulcer disease, who initially presented with a perforated posterior duodenal ulcer following a Billroth II procedure, which was complicated by a duodenal stump abscess and purulent free fluid in the pelvis. The patient subsequently underwent a computed tomography (CT) scan of the abdomen, which revealed extraluminal contrast extravasation within the left upper quadrant, raising concern of an anastomotic leak ( Fig. 1 ). The patient subsequently underwent upper gastrointestinal endoscopy with argon plasma coagulation (APC) and full-thickness endoscopic suturing, with placement of a nasojejunal tube (NJT) in the efferent jejunal limb ( Fig. 2 ; Video 1 ). An upper gastrointestinal series was performed the next day, which showed no evidence of residual leakage ( Fig. 3 ). The patient was discharged with instructions to remain nil by mouth, and an NJT for tube feeding, along with oral antibiotics. Subsequently, she was started on an oral diet and tolerated this without any complications. At follow-up, 3 months after the procedure, the patient was tolerating solid food well.
Computed tomography image of the abdomen showing extraluminal contrast extravasation within the left upper quadrant, raising concern of an anastomotic leak.
Endoscopic views showing the anastomotic leak site: a during suturing; b after endoscopic suturing.
Radiographic image from an upper gastrointestinal series showing no evidence of contrast extravasation, indicating no leakage, and the nasojejunal tube in the efferent limb .
Upper gastrointestinal endoscopy of a chronic anastomotic leak being treated with argon plasma coagulation (APC) and full-thickness endoscopic suturing, with a subsequent upper gastrointestinal series showing no evidence of residual leakage.Video 1
Billroth II (antrectomy with gastrojejunostomy) serves as a surgical management option for perforated gastric ulcers. Anastomotic leakage is a serious complication of Billroth II surgery and occurs 7–10 days after surgery. Surgical intervention is the mainstay of treatment, but may not be amenable for patients who are high risk for morbidity and mortality 1 . While a wide variety of endoscopic therapies exist for the management of leaks, endoscopic suturing has shown clinical success in retrospective studies 1 . This case demonstrates the successful repair of a chronic anastomotic Billroth II leak using APC and endoscopic suturing. Endoscopic suturing is an effective and alternative intervention that can be used for high risk patients who are unable to undergo traditional surgical intervention.
Endoscopy_UCTN_Code_TTT_1AO_2AI
The reference list from the paper itself. Each links out to its DOI / PubMed record.