Enhancing visualization with low echo reduction during endoscopic ultrasound-guided pancreatic duct drainage
Haruka Toyonaga, Tsuyoshi Hayashi, Masayo Motoya, Toshifumi Kin, Kuniyuki Takahashi, Akio Katanuma

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1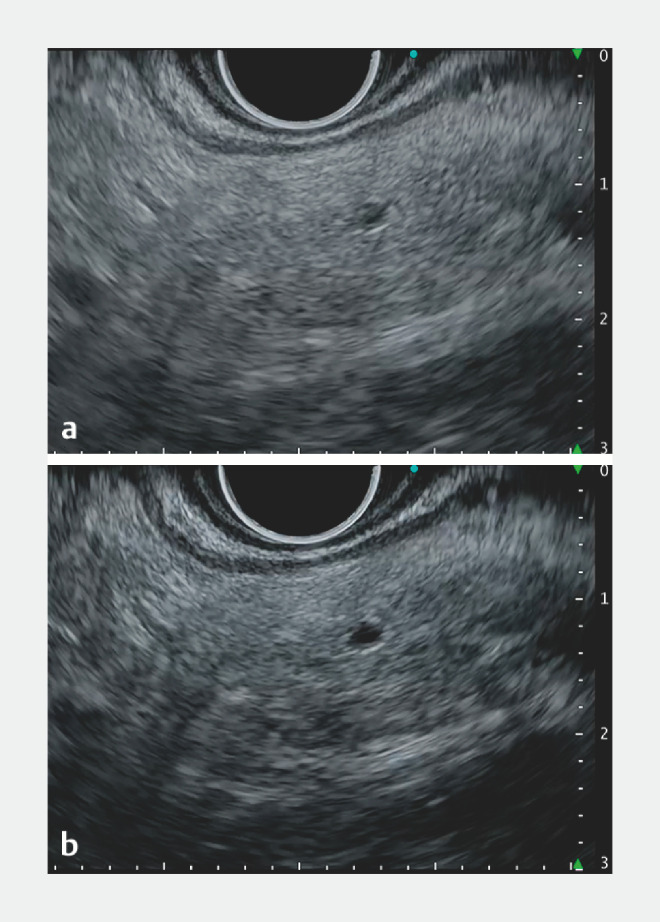 Fig. 2
Fig. 2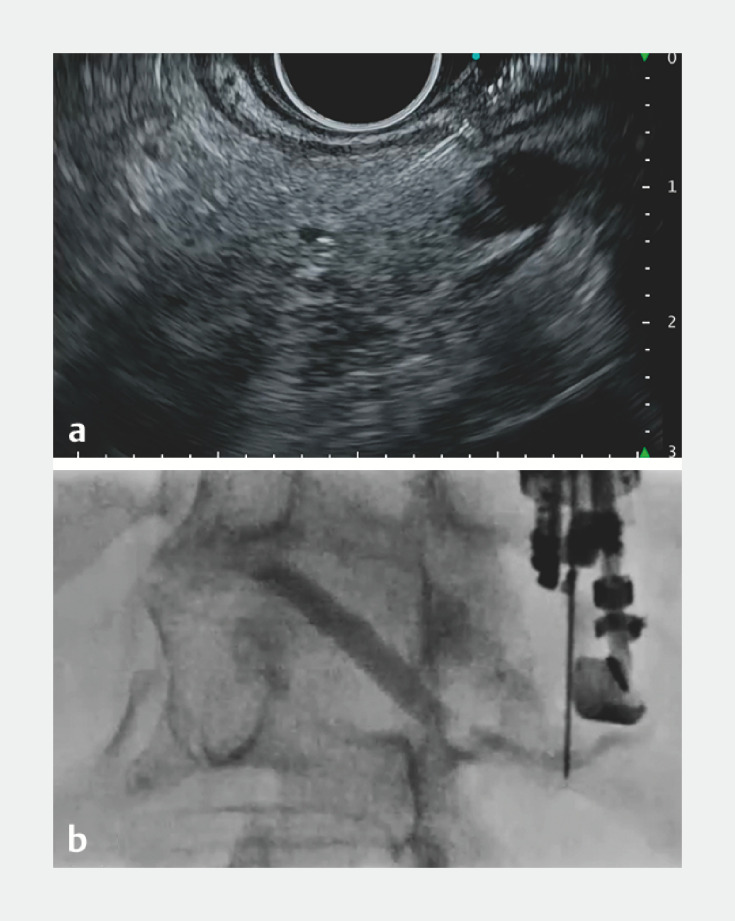 Fig. 3
Fig. 3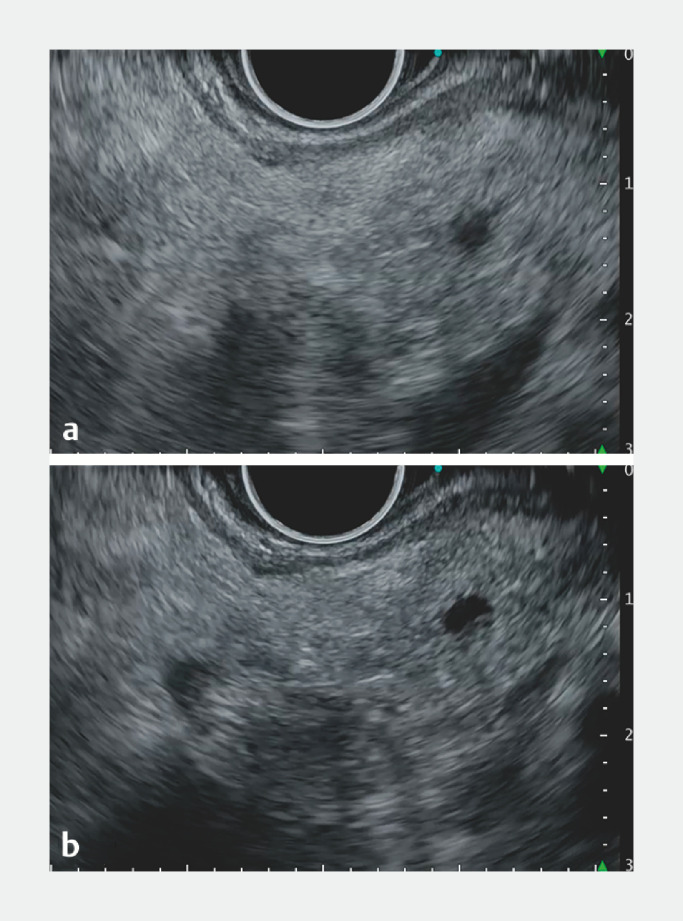 Fig. 4
Fig. 4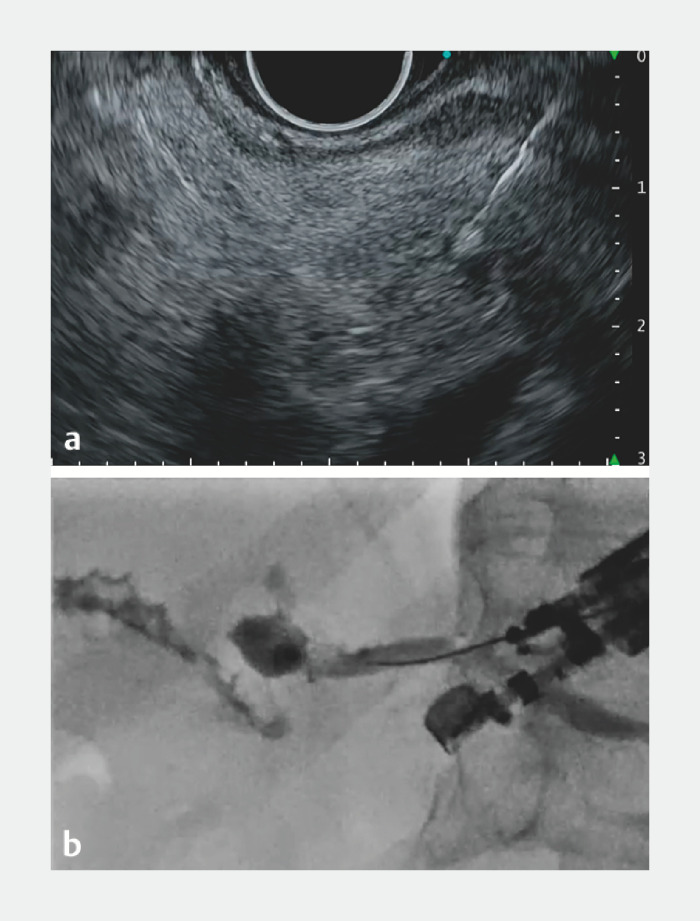 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Gallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments
Endoscopic ultrasound-guided pancreatic duct drainage (EUS-PD) is performed as an alternative when conventional endoscopic pancreatic duct drainage has failed 1 . Although accurately puncturing a narrow pancreatic duct remains challenging, contrast-enhanced EUS has been reported to be effective in puncturing poorly visible ducts 2 3 . Low echo reduction (LER) mode, which is incorporated into a new EUS processor (EVIS EUS EU-ME3; Olympus, Tokyo, Japan), enhances visibility by suppressing low echo signals while maintaining high echo areas 4 5 ; this method may improve EUS-PD outcomes without using contrast media.
In a challenging case of pancreatitis due to pancreaticojejunal anastomotic stenosis after subtotal stomach-preserving pancreaticoduodenectomy ( Fig. 1 ), balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography was unsuccessful due to postoperative adhesions. Hence, EUS-PD was performed using the echoendoscope UCT-260 (Olympus) and EUS processor EU-ME3. To ensure sufficient working space and stent placement distance, we attempted to puncture the upper stream of the pancreatic duct. With a pancreatic duct diameter of just 1.2 mm and poor visibility, puncturing proved challenging. By employing LER, the duct was depicted as a lower echo structure, emphasizing the echo brightness difference with the pancreatic parenchyma, improving visualization ( Fig. 2 , Fig. 3 a ). Successful puncture of the pancreatic duct was achieved using a 22-gauge needle. The nearly perpendicular intersection of the puncture needle and the pancreatic duct posed a challenge in advancing the guidewire ( Fig. 3 b ). After re-evaluating the puncture location ( Fig. 4 ), a spot closer to the anastomosis was punctured, confirmed with contrast, and the guidewire was advanced. After substituting the needle for a catheter and dilating the puncture route ( Fig. 5 ), a 7 Fr × 14 cm plastic stent was placed from the stomach through the pancreatic duct to the jejunum.
Imaging studies of a patient who suffered from pancreatitis due to pancreaticojejunal anastomotic stenosis. a Contrast-enhanced computed tomography. b Magnetic resonance cholangiopancreatography.
Endoscopic ultrasound (EUS) images of the upper stream of the narrow pancreatic duct (1.2 mm in diameter) during EUS-guided pancreatic duct drainage. Low echo reduction (LER) enhances the contrast by suppressing the low echo areas without overemphasizing high echo areas. The LER ranges from Lv.1 to 20 and is usually set at Lv.3. a LER Lv.3 (default). b LER Lv.7 (enhancing).
Puncture of the pancreatic duct. a Endoscopic ultrasound image: low echo reduction enhanced visibility of the narrow pancreatic duct, which the needle then successfully punctured. b Fluoroscopic image: the nearly perpendicular intersection of the puncture needle and the pancreatic duct posed a challenge in advancing the guidewire.
Endoscopic ultrasound (EUS) images of the main pancreatic duct (1.8 mm in diameter) closer to the anastomosis during EUS-guided pancreatography drainage. a Low echo reduction (LER) Lv.3 (default). b LER Lv.7 (enhancing). LER enhanced the contrast without overexposure, and improved visibility of the pancreatic duct.
Successful puncture of the pancreatic duct, contrast of the pancreatic duct and afferent limb, and advancement of the guidewire. Finally, a 7 Fr × 14 cm plastic stent was placed from the stomach through the pancreatic duct to the jejunum after dilation of the puncture route. a Endoscopic ultrasound image. b Fluoroscopic image.
Despite advances in interventional EUS, EUS-PD remains a complex procedure with a high complication rate. LER is a promising image-adjustment feature that may improve visibility and puncture success rates in EUS-PD ( Video 1 ).
Novel low echo reduction modality incorporated into a new endoscopic ultrasound (EUS) processor (EU-ME3; Olympus, Tokyo, Japan), which suppresses low echo areas while maintaining high echo areas to improve the visibility of narrow pancreatic ducts during EUS-guided pancreatic duct drainage.Video 1
Endoscopy_UCTN_Code_TTT_1AS_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1van der Merwe S Wvan Wanrooij RLJ Bronswijk M Therapeutic endoscopic ultrasound: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Endoscopy 20225418520510.1055/a-1717-139134937098 · doi ↗ · pubmed ↗
- 2Minaga K Takenaka M Kamata K Endoscopic ultrasound-guided choledochoduodenostomy with novel use of contrast-enhanced harmonic imaging Endoscopy 201749 E 281e 28228905338 10.1055/s-0043-117939 · doi ↗ · pubmed ↗
- 3Tamura T Kitano M Role of CH-EUS as guidance for EUS-biliary drainage malignant obstruction Minerva Gastroenterol (Torino)20226821021510.23736/S 2724-5985.21.02859-X 33793159 · doi ↗ · pubmed ↗
- 4Toyonaga H Hayashi T Kin T Novel low echo reduction function reduces artifacts in endoscopic ultrasound observation of the gallbladder Endoscopy 202355 E 529E 53110.1055/a-2037-580236894153 PMC 9998231 · doi ↗ · pubmed ↗
- 5Toyonaga H Hayashi T Hama K The application of low echo reduction in endoscopic ultrasound-guided tissue acquisition for pancreatic mass lesions J Hepatobiliary Pancreat Sci 2023301192119510.1002/jhbp.134837658642 · doi ↗ · pubmed ↗