Subxiphoid pericardial drainage for gastric tube ulcer penetrating the pericardium after esophagectomy: A case report
Shinya Ohno, Yoshihiro Tanaka, Yuta Sato, Takayoshi Kato, Kiyoshi Doi, Nobuhisa Matsuhashi

TL;DR
This case report describes a novel surgical technique using subxiphoid pericardial drainage to treat a rare complication of gastric tube ulcers after esophagectomy.
Contribution
The first reported use of subxiphoid pericardial drainage and continuous irrigation lavage for pericardial penetration from a gastric tube ulcer.
Findings
Subxiphoid pericardial drainage and continuous irrigation lavage successfully treated pericardial penetration from a gastric tube ulcer.
The technique prevented septic shock and allowed the patient to recover without complications.
This approach may serve as an effective treatment strategy for similar rare post-esophagectomy complications.
Abstract
Reconstructed gastric tube ulcers are common complications of esophagectomy. When the pericardium is penetrated, digestive juices can cause severe cardiac inflammation, leading to an extremely poor prognosis. We report the first case of pericardial penetration of a constructed stomach tube via the posterior mediastinal route and the first use of subxiphoid pericardial drainage and continuous irrigation lavage. This case involved a 50-year-old woman who underwent an esophagectomy for esophageal cancer nine years prior with gastric tube reconstruction via the posterior mediastinal route. She developed pericardial penetration due to a gastric tube ulcer. Her respiratory and circulatory condition worsened, and pericardial drainage and a prophylactic tracheostomy were performed to prevent septic shock. A 5-cm longitudinal incision was made in the epigastric region, and a 4-cm T-shaped…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
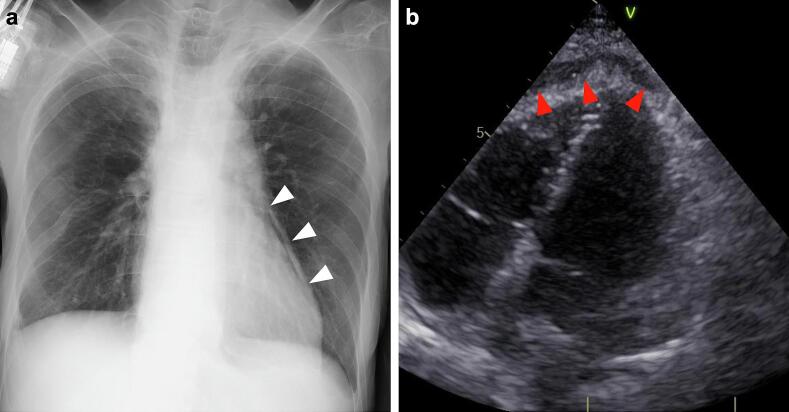 Figure 1
Figure 1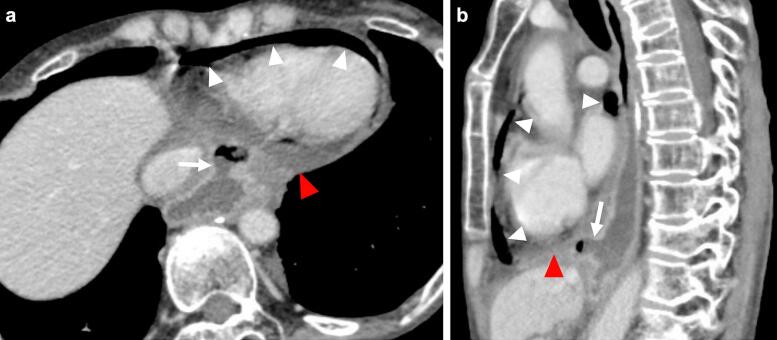 Figure 2
Figure 2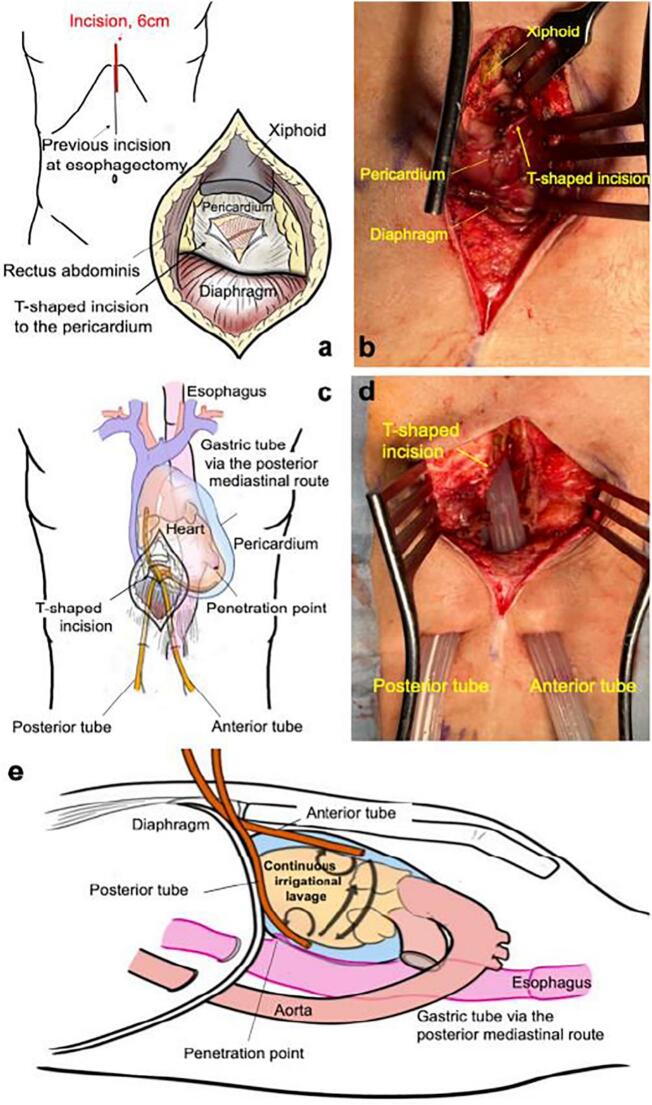 Figure 3
Figure 3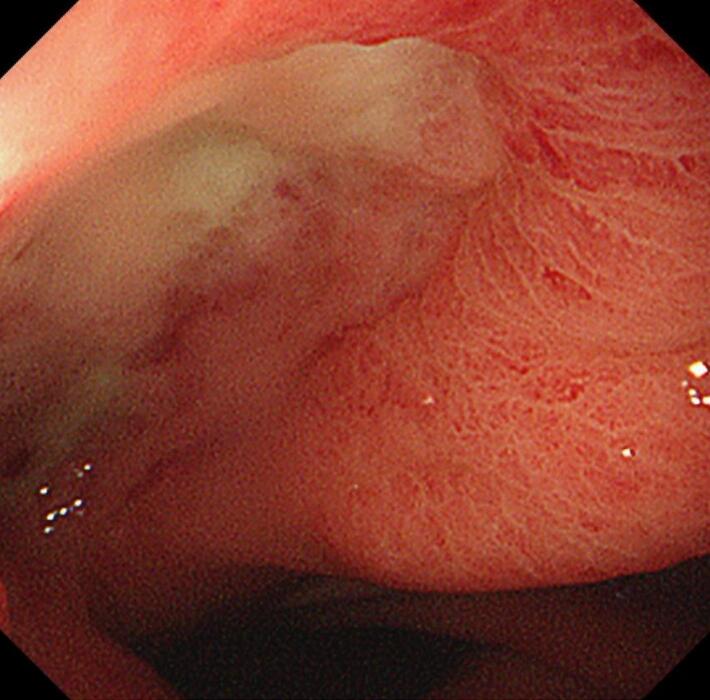 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPleural and Pulmonary Diseases · Pericarditis and Cardiac Tamponade · Pneumothorax, Barotrauma, Emphysema
Introduction
1
When a gastric tube ulcer penetrates the mediastinum, digestive juices drain into the mediastinum, causing severe inflammation. These juices can also penetrate the pericardium, causing severe cardiac inflammation with a poor prognosis (mortality rate of 33–50 %) [1,2].
Subxiphoid pericardial drainage is used in case of pericardium tamponade [3]. Subxiphoid pericardial drainage and continuous irrigation effectively manage gastric tube penetration via the posterior mediastinal route. We describe the first case of pericardial penetration by the gastric tube via the posterior mediastinal route and the use of this management technique. This study was reported in line with the SCARE 2023 criteria [4].
Presentation of case
2
A 50-year-old woman underwent esophagectomy, proximal gastrectomy, and gastric tube reconstruction via the posterior mediastinal route for esophageal cancer. Chemoradiation for the mediastinal lymph nodes recurrence at 8 months after surgery achieved a complete response. Nine years later, the patient presented with chest pain. She had been taking nonsteroidal anti-inflammatory drugs but no proton pump inhibitors.
Chest radiography revealed a pneumopericardium (Fig. 1A), and echocardiography revealed a pericardial effusion (Fig. 1B). Contrast-enhanced computed tomography showed air and fluid in the pericardium and a suspected ulcer in the gastric tube above the diaphragm, confirming the diagnosis (Fig. 2A, B).Fig. 1. Examinations at the time of emergency.(a) Plain radiography revealed pneumopericardium (white arrowheads). (b) Echocardiography showed pericardial effusion (red arrowheads). (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)Fig. 1. Fig. 2Contrast-enhanced computed tomography (CT) images.(a) The axial CT image revealed air (white arrowheads) and fluid (red arrowhead) in the pericardium, and a gastric tube ulcer toward the pericardium (white arrow). (b) The sagittal CT image revealed air (white arrowheads) and fluid (red arrowhead) in the pericardium, and a gastric tube ulcer was located on the diaphragm (white arrow). (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)Fig. 2
Because the patient's respiratory and circulatory condition were unstable, surgical pericardial drainage and prophylactic tracheostomy were performed under general intubated anesthesia. The penetration was located on the dorsal pericardium, and surgery was expected to be difficult due to adhesions, so the patient was treated with subxiphoid pericardial drainage. A 5-cm longitudinal incision was made in the epigastric region, the pericardium was reached via a subxiphoid path from the ventral side of the diaphragm, and a 4-cm T-shaped incision was made through the pericardium (Fig. 3A, B).Fig. 3. Surgical illustrations and intraoperative findings.(a) The illustration of the longitudinal incision in the epigastric region and 4-cm T-shaped incision through the pericardium. (b) The 4 cm T-shaped incision through the pericardium. (c) Illustration after the placement of drains in the anterior and posterior pericardial sac. (d) Two double-lumen tubes were placed in the pericardium through the pericardial T-shaped incision. The right drain was placed in the anterior pericardial sac, and the left was placed in the posterior pericardial sac. (e) Illustration of continuous irrigational lavage via each tube.Fig. 3
Two 20Fr double-lumen drainage tubes, which allowed continuous infusion of the lavage solution, were placed in the anterior and posterior pericardium (Fig. 3C, D). Continuous irrigational lavage with saline solution at 37 °C was initiated at 75 ml/h (Fig. 3E). Candida glabrata was cultured from the pericardial effusion. The patient was treated with micafungin 150 mg/day for 10 days until drainage cultures would be negative findings.
The patient was weaned from the ventilator on postoperative day (POD) 8. On POD 13, an upper endoscopy revealed a gastric tube ulcer but no fistula or cancer recurrence (Fig. 4). On POD 17, continuous irrigation was completed, and the tubes were removed. The patient was discharged on POD 23.Fig. 4. Postoperative upper endoscopy.Postoperative upper endoscopy revealed a gastric tube ulcer but no fistula or cancer recurrence.Fig. 4
Discussion
3
Reconstructed gastric tube ulcers have few subjective symptoms because of the sympathetic nerve transection during creation of the gastric tube [5]; however, they are often only discovered in severe cases. When a gastric tube ulcer penetrates the pericardium, most patients present with symptoms such as fever, chest pain, respiratory distress, and hematemesis [[5], [6], [7], [8]].
Reports of surgical drainage include right thoracotomy [9], left thoracoscopy [8], and median sternotomy [6], all accomplished via the retrosternal route. Surgical drainage via the posterior mediastinal route is difficult because the gastric tube is located on the dorsal side of the pericardium, adhesions from the previous operation are present in the right thoracic cavity, and the descending aorta occupies the left thoracic cavity.
In contrast, subxiphoid pericardial drainage offers the following advantages: it is less invasive than other surgical drainage techniques, the spread of surgical contamination is minimized, and if the patient's condition is good, the technique can be performed under local anesthesia within 30 min [10]. In addition, the creation of a closed space between the pericardium and the drainage tubes allows for closed lavage of the pericardium. Continuous irrigation is useful in controlling chemical inflammation and infections.
With this technique, there is no clear standard criteria for continuous intrapericardial lavage flow rate, however, we should strictly check the drainage volume per 2 h, with special attention paid to avoiding cardiac tamponade. After drainage cultures were negative and fistula closure was confirmed, we determined to cease drainage. Additional surgery may be required if the infection is uncontrolled or fistula closure does not occur.
Conclusion
4
Subxiphoid pericardial drainage and continuous irrigational lavage are effective for pericardial penetration of a constructed stomach tube via the posterior mediastinal route.
Availability of data and materials
Not applicable.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This study was approved by the review board of Gifu University Hospital (Approval no. 2019-170), and informed consent was obtained from the patient.
Funding
None.
Author contribution
Shinya Ohno drafted the manuscript. Shinya Ohno, Yoshihiro Tanaka, Yuta Sato, and Takayoshi Kato performed surgeries. Yoshihiro Tanaka, Yuta Sato, Kiyoshi Doi, and Nobuhisa Matsuhashi provided academic advice.
Guarantor
Yoshihiro Tanaka.
Conflict of interest statement
We have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ubukata H.Nakachi T.Tabuchi T.Nagata H.Takemura A.Shimazaki J.Gastric tube perforation after esophagectomy for esophageal cancer Surg. Today 4120116126192153393110.1007/s 00595-010-4476-9 · doi ↗ · pubmed ↗
- 2Mizuta N.Suganuma T.Nakatani K.Suzuki K.Yonekawa C.Hoshi H.Gastric tube ulcer perforation into the pericardial space after esophagectomy for esophageal cancer managed successfully by emergency surgery Jpn J Gastroenterol Surg 522019137145
- 3Petcu C.P.Droc I.The efficiency of surgical subxiphoid pericardial drainage and percutaneous pericardial drainage in pericardial effusions associated with cardiac tamponade Chirurgia (Bucur).108201322623323618573 · pubmed ↗
- 4Sohrabi C.Mathew G.Maria N.Kerwan A.Franchi T.Agha R.A.The SCARE 2023 guideline: updating consensus Surgical C Ase R Eport (SCARE) guidelines Int J Surg Lond Engl.10952023113610.1097/JS 9.0000000000000373 PMC 1038940137013953 · doi ↗ · pubmed ↗
- 5Sylvin E.A.Jassar A.S.Kucharczuk J.C.Vallabhajosyula P.Pericardial-esophageal fistula: a rare but increasing complication of cardiac ablation Thorac Cardiovasc Surg Rep 112022272910.1055/s-0041-1736209 PMC 890137135265452 · doi ↗ · pubmed ↗
- 6Kato T.Mori T.Niibori K.A case of gastropericardial fistula of a gastric tube after esophagectomy: a case report and review World J. Emerg. Surg.52010202066316710.1186/1749-7922-5-20PMC 2917401 · doi ↗ · pubmed ↗
- 7Yamaguchi H.Kato M.Tada N.Murono K.Ishigami H.Kaisaki S.Gastropericardial fistula resulting from ulcerative perforation of the reconstructed gastric tube after surgery for esophageal cancer Esophagus 82011137141
- 8Watanabe M.Matsuura K.Baba H.Yoshizumi T.Ikegami T.Soejima Y.Thoracoscopic pericardial drainage for gastric tube ulcer penetrated into the pericardium Fukuoka Igaku Zasshi 104201338939324511671 · pubmed ↗