When the second comes first– rhabdomyosarcoma preceding heritable retinoblastoma– a case report
Devjyoti Tripathy, Alexandre Moulin, Jacques Bijon, Carole Gengler, Maja Beck-Popovic, Francis L. Munier, Christina Stathopoulos

TL;DR
A rare case is reported where rhabdomyosarcoma appeared before heritable retinoblastoma in a child, challenging typical disease progression patterns.
Contribution
This case report highlights an atypical sequence of tumor manifestation in a heritable retinoblastoma patient.
Findings
Rhabdomyosarcoma preceded the diagnosis of heritable retinoblastoma in a monozygotic twin.
The child developed metastatic rhabdomyosarcoma and succumbed despite treatment.
This case reverses the usual timeline of second primary tumors in heritable retinoblastoma survivors.
Abstract
Retinoblastoma (rb) is the most frequent intraocular tumor, accounting for 3% of all childhood cancers. Heritable rb survivors are germline carriers for an RB1 mutation and have a lifelong risk to develop non-ocular second primary tumors (SPTs) involving multiple other organs like the bones, soft tissues, or skin. These SPTs usually become manifest several years succeeding the diagnosis of rb. In our instance, however, a non-ocular SPT presented prior to the diagnosis of heritable rb. We report a rare case of a monozygotic twin who presented with primary rhabdomyosarcoma (RMS) preceding the manifestation of heritable rb. The rb was diagnosed when the child developed strabismus while already on therapy for the RMS. The child underwent therapy for both as per defined treatment protocols. The rb regressed well on treatment, but the RMS relapsed and the child developed multiple refractory…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
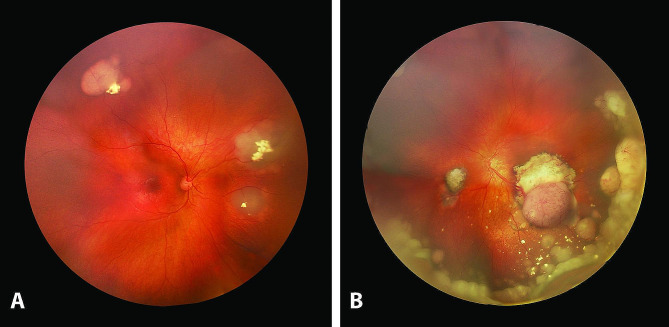 Figure 1
Figure 1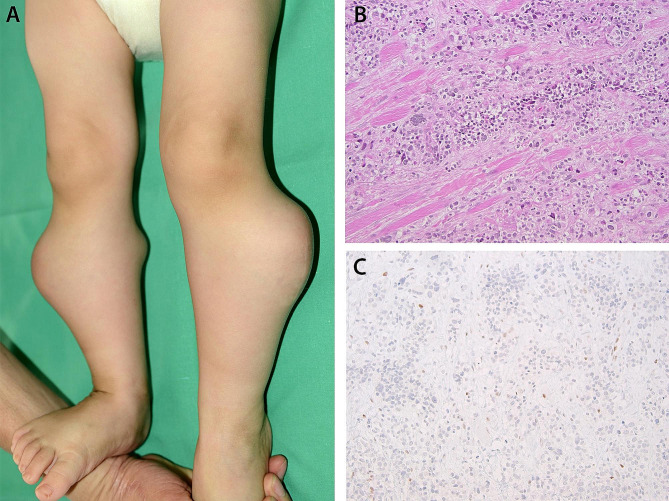 Figure 2
Figure 2- —University of Lausanne
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Oncology and Treatments · Ear and Head Tumors · Sarcoma Diagnosis and Treatment
Background
Retinoblastoma (rb) is the most frequent intraocular tumor, accounting for 3% of all childhood cancers. Retinoblastoma survivors with a germline RB1 mutation are at lifetime risk to develop various types of non-ocular second primary tumors (SPTs) in diverse anatomic locations, such as the bones, the soft tissue or the skin [1]. This risk is further increased after external beam radiotherapy and, to a lesser extent, chemotherapy [2]. Herein we report a rare case of a monozygotic twin presenting with primary rhabdomyosarcoma preceding the diagnosis of heritable rb.
Case presentation
A 14-month-old boy developed left eye strabismus following sustentacular systemic vinblastine, cyclophosphamide, and local radiotherapy for an alveolar RMS (PAX3-FOXO1 positive) of the right buttock diagnosed elsewhere at the age of 5 months. Previous treatments included systemic polychemotherapy (carboplatin, doxorubicin, vincristine, ifosfamide, etoposide and actinomycin) (CWS-2009 protocol), five cycles given prior, and four after incomplete surgical resection of the tumor. Ophthalmic evaluation revealed bilateral rb, that was also present in the younger asymptomatic monozygotic fellow twin. Fundus examination of the 3-year older brother and the parents was normal. Both twins were referred to Lausanne for further treatment. Examination under anesthesia of the elder one revealed three partially regressed tumors in the right eye (OD) and two relapsing tumors in the left eye (OS) associated with diffuse subretinal seeding, consistent with International Intraocular Retinoblastoma Classification (IIRC) Group B in OD and group D in OS (Fig. 1). Intraocular tumor regression was achieved with one intra-arterial melphalan (3.7 mg) in OS and bilateral focal treatments (5 sessions of cryotherapy and/or thermotherapy given over 5 months). However, about a year following the diagnosis of rb, the child unfortunately developed refractory multifocal metastatic RMS involving both lower extremities (Fig. 2A), the lungs, and the brain confirmed on histopathology and immunostaining (Fig. 2B, C), and succumbed to his disease. The fellow twin had rb IIRC group B in OD and group D in OS treated with one cycle of systemic chemotherapy followed by three intra-arterial melphalan in OS together with bilateral focal treatments and remained tumor-free at 6 years follow-up.
Fig. 1. Fundus pictures of a 14-month-old boy developing strabismus of the left eye while under systemic chemotherapy for an alveolar RMS with the right eye showing three partially regressed endophytic tumors with focal intralesional calcifications (A) and the left eye showing two relapsing tumors with diffuse subretinal seeding reaching the inferior ora serrata (B)
Fig. 2. Bilateral nodular multifocal deformations of both lower extremities from alveolar RMS metastases (A) confirmed on histopathology showing nests and sheets of undifferentiated round tumor cells with rhabdoid features infiltrating the striated muscle (hematoxylin and eosin, magnification X126) (B). Immunostaining of the tumor tissue displaying RB1 loss in most of the tumor nuclei (magnification X126) (C)
Both twins were found to be carriers of a RB1 loss of function mutation (NM_000321.2:c.1128-1G > A:p.(Thr377 Leufs*3). The father was a 10% mosaic healthy carrier.
Discussion and conclusions
Most rb patients are diagnosed before the age of 3 years, those with a known family history of rb and bilateral rb being diagnosed usually earlier than the unilateral form (4 months and 12 months respectively versus 24 months) [3]. Germline carriers for a RB1 mutation have a 3.2% risk to develop a midline intracranial tumor (MIT) (most commonly a pinealoblastoma) referred to as trilateral rb and a lifelong risk to develop SPTs which cumulative incidence is reported to be 3.7% at the age of 10 years and 17.7% at the age of 35 years [4, 5]. The most prevalent SPTs are sarcoma (68%) followed by carcinoma (14%) and melanoma (8%) [1]. In contrast to MIT that can occur before or at time of the rb diagnosis-, other SPT cases follow the rb diagnosis, with a latency ranging 1–55 years [1].
Rhabdomyosarcoma is the most common soft tissue sarcoma in children, accounting for about 3% of childhood cancers [6]. In rb survivors, rhabdomyosarcoma is the second most frequent sarcoma after osteosarcoma with over 85% of cases occurring in the head and neck within the field of irradiation [1]. Alveolar RMS is a subtype of RMS with an incidence of 1 per million children and adolescents. Most cases occur sporadically with no genetic predisposition and are associated with a balanced chromosomal translocation t(2;13)(q35;q14) or t(1:13)(p36;q14) generating the PAX3 or PAX7-FOXO1 fusion variant exhibiting oncogenic activity [6]. Alveolar RMS most commonly presents in the pediatric and adolescent age group (typically between 10 and 20 years), which is at a later age compared to its commoner counterpart embryonal RMS (presenting typically between birth and 5 years), and is known to have a predilection for the extremities and the perineal region [7].
Herein we report a case of bilateral rb, partially regressed during systemic chemotherapy given for an alveolar RMS, which only became symptomatic on relapse once the systemic polychemotherapy was stopped. Though of extremely rare occurrence, this case illustrates that a non-ocular SPT may manifest at an unusually early age in a patient with heritable rb and may precede the diagnosis of the rb itself. The awareness of this possibility may be of help to onco-pediatricians involved with the management of such cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Woo KI Harbour JW Review of 676 second primary tumors in patients with retinoblastoma: association between age at onset and tumor type Arch Ophthalmol 201012878657010.1001/archophthalmol.2010.12620625047 · doi ↗ · pubmed ↗
- 2Temming P Arendt M Viehmann A Incidence of second cancers after radiotherapy and systemic chemotherapy in heritable retinoblastoma survivors: a report from the German reference center Pediatr Blood Cancer 2017641718010.1002/pbc.2619327567086 · doi ↗ · pubmed ↗
- 3Dimaras H Corson TW Cobrinik D Retinoblastoma Nat Rev Dis Primers 201511502110.1038/nrdp.2015.2127189421 PMC 5744255 · doi ↗ · pubmed ↗
- 4de Jong MC Kors W Ade Graaf P Trilateral retinoblastoma: a systematic review and meta-analysis Lancet Oncol 2014151011576710.1016/S 1470-2045(14)70336-525126964 · doi ↗ · pubmed ↗
- 5Moll AC, Imhof SM, Bouter LM, et al. Second primary tumors in patients with hereditary retinoblastoma: a register-based follow-up study, 1945–1994. Int J Cancer. 1996;67(4):515–9. 10.1002/(SICI)1097-0215(19960807)67:4%3C 515::AID-IJC 9%3E 3.0.CO;2-V.10.1002/(SICI)1097-0215(19960807)67:4<515::AID-IJC 9>3.0.CO;2-V 8759610 · doi ↗ · pubmed ↗
- 6Skapek SX Ferrari A Gupta AA Rhabdomyosarcoma Nat Rev Dis Primers 201951110.1038/s 41572-018-0051-230617281 PMC 7456566 · doi ↗ · pubmed ↗
- 7Agaram NP Evolving classification of rhabdomyosarcoma Histopathology 20228019810810.1111/his.1444934958505 PMC 9425116 · doi ↗ · pubmed ↗