Unusual Presentation of Primary Pulmonary Sarcomatous Cancer With Brain Metastasis: A Case Report
Leena Alhusari, Ihab Tahboub, Moh'd Masoudi, Logan M Lawrence, Muhammad Jamil

TL;DR
A 79-year-old woman with rare lung cancer developed brain metastases shortly after diagnosis, highlighting the aggressive nature and poor prognosis of this cancer subtype.
Contribution
This case report highlights the unusual progression of primary pulmonary sarcomatous cancer to brain metastasis and its clinical implications.
Findings
Brain metastasis in sarcomatous lung cancer is rare and occurs at later stages.
The patient's disease progressed rapidly to brain metastasis despite initial absence of intracranial lesions.
Treatment options for this aggressive cancer subtype are limited and prognosis remains poor.
Abstract
Pulmonary sarcomatous carcinoma is a rare subtype of non-small cell lung cancer (NSCLC). This cancer has very low survival rates primarily due to its aggressive nature and propensity for early spread to abdominal organs and the skeletal system. Remarkably, brain metastasis is observed at later stages of the disease, likely attributing to the high fatality rate after the disease progresses to the brain tissue. In our case, a 79-year-old female with a 45-pack-year smoking history sought medical attention at a primary care clinic due to a 3-month history of recurrent right-sided chest pain. Notably, she denied cough, sputum production, palpitations, or syncope. CT chest revealed a 6.8 x 3.5 cm mass in the right upper lobe (RUL) of the lung, with evidence of obstruction and infiltration of the adjacent chest wall. A PET scan indicated increased uptake in the mass and the presence of smaller…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
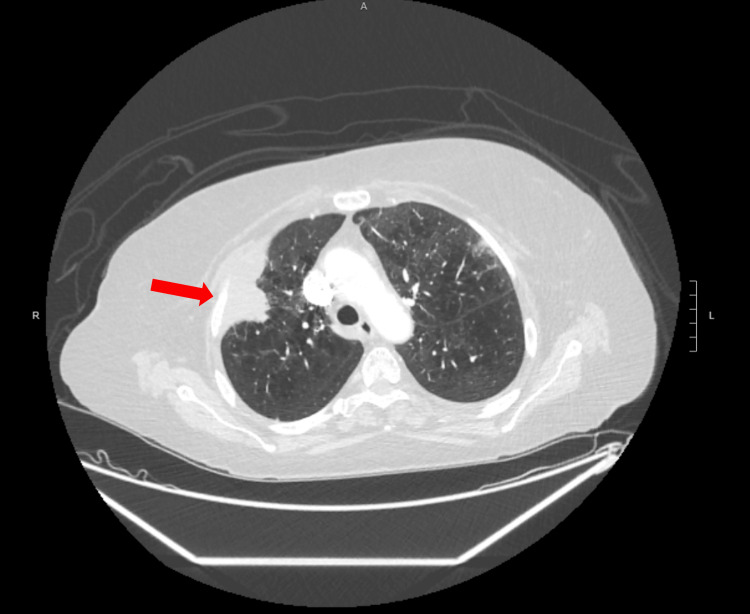 Figure 1
Figure 1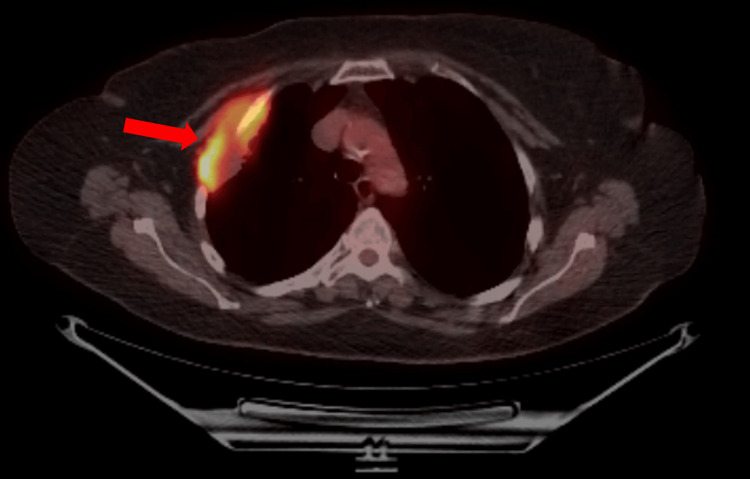 Figure 2
Figure 2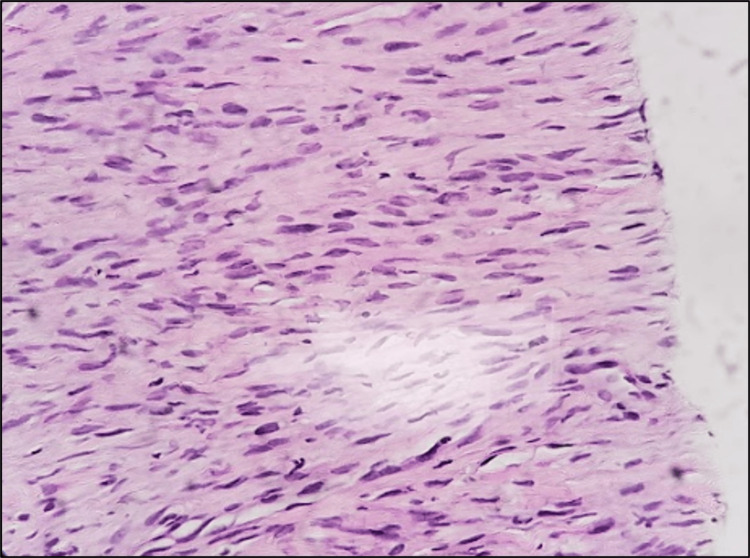 Figure 3
Figure 3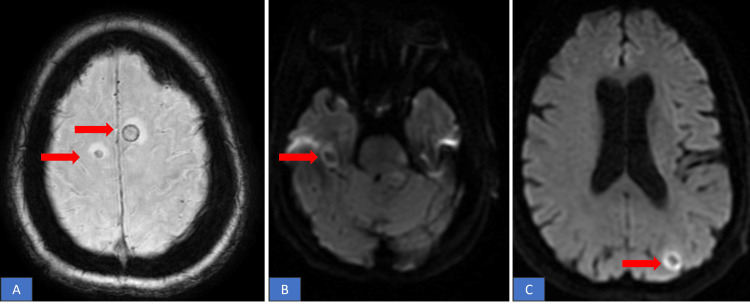 Figure 4
Figure 4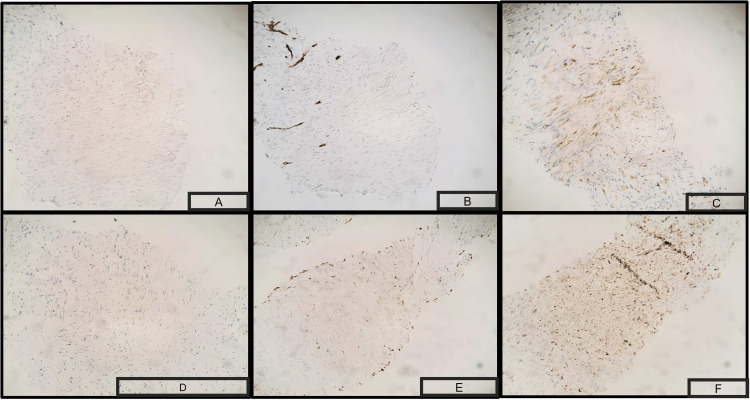 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetastasis and carcinoma case studies · Cancer Diagnosis and Treatment · Lung Cancer Diagnosis and Treatment
Introduction
Sarcomatous carcinoma of the lung is a seldom encountered subtype of non-small cell lung cancer (NSCLC), constituting approximately 0.5% of all NSCLC cases [1,2]. Our case is consistent with the fact that this malignancy has an aggressive metastatic potential, resulting in a dismal prognosis, with a 5-year survival rate of merely 15-20% and a median survival duration of approximately 10 months [3,4]. The metastatic cells display a remarkable ability to disseminate through both lymphatic and blood vessels, giving rise to secondary tumors in various distant sites, including the gastrointestinal tract, kidneys, bones, and adrenal glands [5]. Notably, brain metastasis is unusual and considered a premature presentation in the sarcomatous variant of NSCLC. In this report, we present a compelling case of primary pulmonary sarcomatous carcinoma, characterized by its rapid metastasis to the brain.
Case presentation
A 79-year-old Caucasian woman with a notable history of 45-pack-year smoking, chronic hypertension, and dyslipidemia, sought care at the clinic due to persistent right-sided chest pain for the last three months. Despite trying over-the-counter antacids, her symptoms had not improved significantly. She did not report any other respiratory issues, including cough, sputum production, palpitations, syncope, or constitutional symptoms. Radiological examinations, comprising a chest X-ray and subsequent chest CT scan, unveiled a peripheral mass in the right upper lobe (RUL) of the lung, measuring 6.8 x 3.5 cm, with evidence of infiltration into nearby chest wall structures, encompassing the pectoralis minor muscle and adjacent rib (Figure 1). A PET scan exhibited heightened uptake in the RUL mass and smaller bilateral pulmonary nodules (Figure 2).
Chest CT scan showing a 6.8 x 3.5 cm mass in the right upper lobe of the lung
A PET scan showed increased uptake in the RUL mass
The PET scan additionally detected heightened uptake in multiple nodules situated in the left upper arm, abdomen, right inguinal region, left thigh, and cecum. Intriguingly, no intracranial lesions were observed. To explore the abdominal nodules further, a colonoscopy was conducted, yielding benign findings. A CT-guided biopsy of the lung mass unveiled a moderately cellular and pleomorphic spindle cell proliferation, featuring focal necrosis and ovoid nuclei with dense chromatin. These characteristics were consistent with a diagnosis of sarcomatous cancer (Figure 3).
H&E stain showing solid sheets of moderately cellular pleomorphic spindle cell proliferation, focally necrotic. The spindle cells show an ill-defined cytoplasm and an ovoid nucleus with dense chromatin.
Three days later, the patient revisited the clinic, reporting numbness and tingling in her lower extremities. Notably, she denied experiencing any other neurological symptoms, such as weakness, dizziness, imbalance, visual issues, or urinary or bladder incontinence. As part of the outpatient evaluation, an MRI of the brain revealed the presence of multiple bilateral brain metastases accompanied by vasogenic edema(Figure 4). The patient was admitted to the hospital for further assessment of these brain metastases and treated with steroids to alleviate the edema. Subsequently, the pathology was meticulously reviewed at Mayo Clinic, ultimately reaffirming the diagnosis of primary pulmonary sarcomatous carcinoma and was corroborated by the positive staining of tumor cells for pan-cytokeratin (AE1/AE3), CK7, and epithelial membrane antigen (Figure 5).
(a,b,c) MRI brain showing multiple enhancing foci noted bilaterally consistent with brain metastases.
Tissue biopsy of the lung cancer testing positive for Immunostains suggestive of pulmonary sarcomatous cancer. A) positive S100 stain, B) positive p40 stain, C) cells positive for CD34 , D) cells positive for smooth muscle actin, E) positive Desmin stain, F) positive TTF-1.
The patient underwent whole-brain radiation therapy followed by treatment with Nab-paclitaxel, carboplatin, and atezolizumab. Unfortunately, the patient encountered substantial treatment-related side effects, prompting a transition to single-agent immunotherapy involving pembrolizumab. After receiving a sole dose of pembrolizumab, the patient decided to discontinue aggressive treatment and opted for hospice care. Tragically, she passed away just 13 days later.
Discussion
Sarcomatous carcinoma of the lung is distinguished by histological features reminiscent of sarcomas, marked by poorly differentiated cells with a spindle/giant-like appearance. The emergence of the sarcomatoid component in these tumors is believed to stem from cellular metaplasia secondary to the activation of an epithelial-mesenchymal transition program in a process called conversion paradigm [6]. The predominant carcinomatous component is typically squamous cell carcinoma (69%), followed by adenocarcinoma (20%), with large cell carcinoma being less frequent (11%) [7]. Primary pulmonary sarcomatous carcinoma (PSC) encompasses five major histological variants: pleomorphic, spindle cell, giant cell, carcinosarcoma, and pulmonary blastoma [8].
PSC is an exceedingly rare entity, representing less than 0.5% of all lung cancers [2]. Gender and heavy smoking are considered risk factors for the development of PSC with a male-to-female ratio of approximately 7:1 and occurring at a median age of 65 years [9]. The existing literature primarily relies on a limited number of case series and retrospective studies [10] hence, making it challenging to establish definitive clinical characteristics, diagnosis, treatment strategies, and survival outcomes [11].
PSC can manifest on imaging as a central mass with an endobronchial polypoid appearance or as a large peripheral mass with well-defined margins, often featuring necrotic, hemorrhagic areas, and occasionally cavitation [12]. Information regarding fluorodeoxyglucose (FDG) uptake in PET-CT imaging for these tumors is limited, with reports indicating significantly higher uptake compared to other lung cancer types or mentioning a maximum standardized uptake value (SUV) of 4.1 [13]. Tissue sampling of central masses are obtained endoscopically compared to transthoracic needling for peripheral lesions [14]. Obtaining a preoperative tissue diagnosis poses challenges due to the tumor's heterogeneity, as biopsies frequently represent only a single facet of the tumor [14]. Immunohistochemistry plays a pivotal role in PSC diagnosis. The histologic features include the presence of spindle or giant cells, along with at least 10% of the tumor mass exhibiting adenocarcinoma or squamous cell features [14]. PSC is associated with specific gene mutations (e.g., KRAS, P53, C-MET) which contribute to tumor aggression, frequent metastasis, and resistance to chemotherapy and tyrosine kinase inhibitors [8,12]. PD-L1 overexpression is often associated with the transition from adenocarcinoma histology to PSC [12].
The standard therapeutic approach for PSC remains undetermined due to its low incidence [15]. Sarcomas, including pulmonary sarcoma, often display resistance to chemotherapy with toxic chemotherapy being less effective compared to other sub-types of NSCLC. Hence, complete surgical resection is considered the most favorable treatment for early-stage PSC patients [16-18]. Alongside surgical intervention, radiation therapy is well-established and effective when combined with surgery [14]. While surgical resection can lead to long-term survival, considering adjuvant therapy is prudent due to the tumor's aggressive nature [19]. Chemotherapeutic agents such as doxorubicin, adriamycin, ifosfamide, and dacarbazine have proven effective. In cases of distant metastases, combination chemotherapy is recommended. Brain metastasis in sarcomatous lung cancer is relatively rare when compared to other types of non-small cell lung cancer (NSCLC) and other lung cancer subtypes. Recently introduced targeted therapies, such as those targeting epidermal growth factor receptor (EGFR) mutations and programmed cell death ligand-1 (PD-L1), have shown promise in individual cases [12].
Brain metastasis is found in roughly 3.3% of patients with sarcomas originating from skeletal or soft tissue, and the percentage is even lower when dealing with primary pulmonary sarcoma. Managing sarcomatous lung cancer with brain metastasis necessitates a multidisciplinary approach, involving surgery, radiation therapy, chemotherapy, targeted therapy, and immunotherapy, contingent upon the specific tumor characteristics and the patient's overall health [12]. Unfortunately, the prognosis for sarcomatous lung cancer with brain metastasis remains generally unfavorable, signifying an advanced stage of the disease with limited treatment options.
Conclusions
Primary pulmonary sarcomatous carcinoma (PSC) stands as an infrequent subtype of NSCLC, characterized by a grim prognosis. Brain metastasis in sarcomatous lung cancer signifies an advanced disease stage. Diagnosing PSC can be intricate, necessitating extensive workup and immunohistochemistry for definitive confirmation. Encouragingly, targeted therapies and immunotherapy display the potential for enhancing PSC treatment outcomes, particularly in cases with specific mutations and PD-L1 expression. Further research and larger-scale studies are imperative to gain deeper insights into the molecular characteristics and optimize treatment strategies for this aggressive variant of lung cancer.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sarcomatoid carcinoma of the lung: histologic criteria and common lesions in the differential diagnosis Arch Pathol Lab Med Franks TJ Galvin JR 495413420102007360510.5858/2008-0547-RAR.1 · doi ↗ · pubmed ↗
- 2Pulmonary sarcomatoid carcinoma: An analysis of the National Cancer Data Base Clin Lung Cancer Steuer CE Behera M Liu Y 2862921820172804377310.1016/j.cllc.2016.11.016 · doi ↗ · pubmed ↗
- 3Sarcomatoid carcinoma of the lung: The Mayo Clinic experience in 127 patients Clin Lung Cancer Maneenil K Xue Z Liu M 03319201810.1016/j.cllc.2017.12.00829454534 · doi ↗ · pubmed ↗
- 4A resected case of pulmonary carcinosarcoma Ann Thorac Cardiovasc Surg Goto T Maeshima A Tajima A Kato R 190193162010 https://pubmed.ncbi.nlm.nih.gov/20930681/20930681 · pubmed ↗
- 5Sarcomatoid lung carcinomas show high levels of programmed death ligand-1 (PD-L 1)J Thorac Oncol Velcheti V Rimm DL Schalper KA 803805820132367655810.1097/JTO.0b 013e 318292 be 18PMC 3703468 · doi ↗ · pubmed ↗
- 6Review article: pulmonary sarcomatoid carcinomas: a practical overview Int J Surg Pathol Pelosi G Sonzogni A De Pas T 1031201820101912445210.1177/1066896908330049 · doi ↗ · pubmed ↗
- 7Pulmonary carcinosarcoma: Diagnostic problems and determinants of the prognosis Eur J Cardiothorac Surg Huwer H Kalweit G Straub U Feindt P Volkmer I Gams E 403407101996881713310.1016/s 1010-7940(96)80105-9 · doi ↗ · pubmed ↗
- 8Sarcomatoid carcinoma of the lung with brain metastases J Bras Pneumol Oliveira MF Watanabe SC Andrade MP Rotta JM Pinto FC 7537563920132447377110.1590/S 1806-37132013000600016 PMC 4075908 · doi ↗ · pubmed ↗