Atypical vascular lesions cleared with Mohs micrographic surgery
Jose L. Cortez, Hillary Elwood, Andrew Matsumoto

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
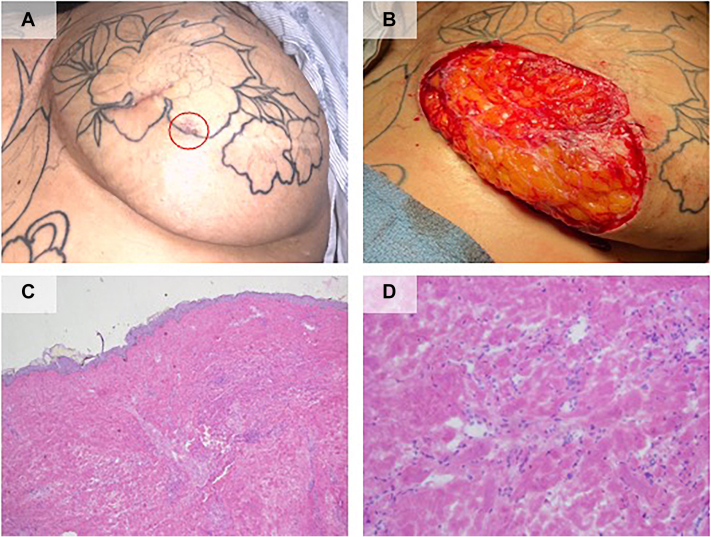 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Tumors and Angiosarcomas · Cutaneous lymphoproliferative disorders research · Nonmelanoma Skin Cancer Studies
Introduction
Atypical vascular lesions (AVLs) in patients having undergone treatment for breast cancer have been described microscopically as dilated vascular spaces that often present 1-6 years after a patient undergoes radiation therapy.1^,^2 AVLs are considered benign lesions that exist on a spectrum with malignant angiosarcoma.3 It is unclear whether AVLs represent precursor lesions to angiosarcomas or are an independent risk factor for developing angiosarcoma.4 The application of Mohs surgery can be considered to achieve clear margins in select cases. Here, we describe a case of AVLs arising on a patient’s chest following radiation therapy for breast cancer cleared with Mohs micrographic surgery.
Case report
A 33-year-old female with a history of estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2 positive left breast invasive ductal carcinoma diagnosed and treated in 2016 was evaluated by dermatology for treatment of atypical vascular lesions with Mohs surgery.
In 2017, the patient underwent neoadjuvant chemotherapy, bilateral skin sparing mastectomy with two-stage tissue expander reconstruction, and adjuvant radiation therapy. She completed her reconstruction with bilateral deep inferior epigastric artery perforator flaps that same year. In July 2022, the patient reported new skin lesions on the inferior/medial left reconstructed breast that were biopsied and found to be atypical vascular lesions. Given concern for risk of transformation to angiosarcoma, she subsequently underwent 2 excisions in September 2022 and November 2022 with surgical oncology with positive margins. The patient was presented at her hospital’s tumor board who recommended complete resection of the AVLs and close surveillance. The patient then underwent a third excision in March 2023 with plastic surgery, and margins were again positive. She was then referred to our Mohs surgery clinic for consideration of treatment with Mohs surgery.
The patient was first evaluated by dermatology in April 2023 and at the time was noted to have telangiectasias overlying the sternum/between the breasts, with multiple well healed surgical scars and purpuric plaque at the lateral and inferior edge of her most recent scar on the left breast, Fig 1, A. After discussion of treatment options, she underwent Mohs surgery with intraoperative histopathology demonstrating persistence of vascular ectasias/atypical vascular lesions with characteristic hobnailed endothelial cells, Fig 1, C and D. After 6 stages, a clear margin was achieved with a final defect size of 8.5 x 9.5 centimeters, Fig 1, B. Repair was performed by the referring plastic surgeon with full-thickness skin graft reconstruction of the defect.Fig 1. Clinical images. A, Left breast demonstrating well healed prior excision scars and dusky, cigarette burn, atrophic papules and plaques (red circle). B, Left breast defect measuring 8.5 × 9.5 centimeters in size with clear margins after 6 stages of Mohs micrographic surgery. Histopathology. Frozen sections stained with hematoxylin and eosin demonstrating atypical ectatic vessels in the dermis with hobnailed endothelial cells projecting into the lumina (C) scan and (D) 20× magnification.
Discussion
AVLs were first described by Fineberg et al. as focal proliferations of dilated vascular spaces in 4 patients who had undergone radiation therapy for breast carcinoma.5 These lesions were further defined by Brenn et al and Patton et al in 2005 and 2008, respectively. Clinically, AVLs present as flesh-colored to erythematous/violaceous papules or nodules to plaques most commonly on the chest wall 1-6 years after radiation therapy.1^,^2
There are 2 histologic subtypes of AVLs described in the literature, a lymphatic and vascular type. Lymphatic AVLs are composed of predominantly thin-walled lymphatic vessels present in the superficial to mid-dermis.2^,^4 In contrast, vascular AVLs consist of superficial small capillary-sized vessels lined by hobnailed endothelial cells with extravasated red blood cells and hemosiderin, and a surrounding lymphatic component.2^,^4 Both types of AVLs are thought to arise secondary to vascular obstruction from radiation therapy and surgery, resulting in dilation of vessels.4 The dilated vessels present within or adjacent to the area of radiated skin and are thought to be contiguous though this has not been explicitly described in the literature.6
AVLs and angiosarcomas exist on a spectrum, with AVLs often being indistinguishable from well-differentiated angiosarcomas.3 While AVLs have a benign course, angiosarcoma has a very high mortality, so it is important to distinguish between these 2 entities. It is unclear if AVLs represent a true precursor to angiosarcoma, or whether this entity is simply an independent risk factor for the development of secondary angiosarcoma.4 However, there have been reports of AVLs progressing to angiosarcoma after repeated recurrences of AVLs.7
Given the potential for malignant transformation, it is often recommended that AVLs be treated definitively to achieve clear margins and followed closely for recurrence. Often, resection of the entire radiation field is required which can result in a large defect, and margins are not always clearly defined.8 for example, a case report by Yoon et al described a patient treated with radiation therapy for a peripheral nerve-sheath tumor, who was found to have AVLs outside the field of radiation exposure.9 Finally, there are few reported cases of good outcomes following Mohs surgery for angiosarcoma. A review by Rodriguez-Jimenez et al. states that over the last century only 1 patient has remained relapse free following Mohs for angiosarcoma, while all other patients had relapsed.10 Therefore, Mohs surgery can be considered as potential treatment modality to ensure clear margins in areas of concern, though should be utilized judiciously as this would not be appropriate for all cases of AVLs.
Herein, we describe a case of a patient with a history of breast cancer that underwent mastectomy and radiation therapy, and developed AVLs in her left reconstructed breast and subsequently underwent Mohs surgery for clearance of her lesions. Mohs surgery can be considered as a treatment modality for AVLs given the potential for significant subclinical spread. Mohs surgeons should be aware of this pathology and the risk of malignant potential to angiosarcoma.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brenn T.Fletcher C.D.M.Radiation-Associated cutaneous atypical vascular lesions and angiosarcoma Am J Surg Pathol 298200598399610.1097/01.PAS.0000156664.04955.8316006792 · doi ↗ · pubmed ↗
- 2Patton K.T.Deyrup A.T.Weiss S.W.Atypical vascular lesions after surgery and radiation of the breast: a clinicopathologic study of 32 cases analyzing histologic heterogeneity and association with angiosarcoma Am J Surg Pathol 326200894395010.1097/PAS.0B 013E 31815 BF 8FE 18551753 · doi ↗ · pubmed ↗
- 3Mattoch I.W.Robbins J.B.Kempson R.L.Kohler S.Post-radiotherapy vascular proliferations in mammary skin: a clinicopathologic study of 11 cases J Am Acad Dermatol 571200712613310.1016/j.jaad.2006.10.02517572278 · doi ↗ · pubmed ↗
- 4Rutland C.D.Bean G.R.Charville G.W.Contemporary diagnostic approach to atypical vascular lesion and angiosarcoma Semin Diagn Pathol 404202328429410.1053/J.SEMDP.2023.04.01737121782 · doi ↗ · pubmed ↗
- 5Fineberg S.Rosen P.P.Cutaneous angiosarcoma and atypical vascular lesions of the skin and breast after radiation therapy for breast carcinoma Am J Clin Pathol 1026199475776310.1093/AJCP/102.6.7577801888 · doi ↗ · pubmed ↗
- 6Anzalone C.L.Cohen P.R.Tschen J.A.Mac Farlane D.F.Radiation-associated atypical vascular lesions: vascular lesions with endothelial cell atypia presenting in the radiation port of breast cancer patients Skinmed 126201434434825823080 · pubmed ↗
- 7Fraga-Guedes C.Gobbi H.Mastropasqua M.G.Clinicopathological and immunohistochemical study of 30 cases of post-radiation atypical vascular lesion of the breast Breast Cancer Res Treat 1462201434735410.1007/S 10549-014-3020-924943869 · doi ↗ · pubmed ↗
- 8Sener S.F.Milos S.Feldman J.L.The spectrum of vascular lesions in the mammary skin, including angiosarcoma, after breast conservation treatment for breast cancer J Am Coll Surg 19312001222810.1016/S 1072-7515(01)00863-811442250 · doi ↗ · pubmed ↗