Association Between ALK Rearrangement and Ultra-Late Recurrence in Lung Cancer: Case Report and Pooled Analysis
Jamila Mammadova, Tawee Tanvetyanon

TL;DR
This paper reports a rare case of ultra-late lung cancer recurrence and finds that ALK rearrangement is a significant predictor of recurrence timing.
Contribution
The study identifies ALK rearrangement as a novel predictor of ultra-late recurrence in non-small cell lung cancer.
Findings
A case of ultra-late recurrence in a lung cancer patient was reported with EGFR exon 20 insertion.
Multivariable analysis showed ALK rearrangement significantly predicts time to recurrence in NSCLC.
Ultra-late recurrence is rare and occurs more than 10 years after initial treatment.
Abstract
Ultra-late recurrence, defined as recurrence occurring 10 years or longer after curative treatment, is uncommon for non-small cell lung cancer (NSCLC). To date, factors associated with ultra-late recurrence remain unknown. We report a case with ultra-late recurrence and reviewed the literature published during 2010-2023. This is a case of a 66-year-old woman, with a significant smoking history and a previous history of lung adenocarcinoma, who underwent surgery for a brain metastasis detected on imaging. The pathology confirmed lung adenocarcinoma with an epidermal growth factor receptor (EGFR) exon 20 insertion, a finding consistent with the initial lung surgery a decade ago. With receiving intrathecal topotecan, the patient has maintained stable disease 10 months post-surgery. Given the rarity of ultra-late recurrence of NSCLC, we also conducted a pooled analysis with the outcome of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1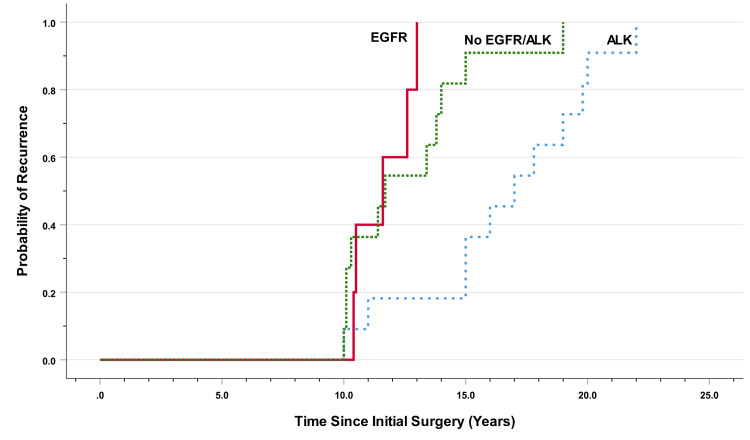 Figure 2
Figure 2| Patient number | First author, year [reference] | Sex | Age (years) | Time to recurrence (years) | Smoking history | Initial stage | Biomarker status |
| 1 | Inaoka, 2010 [ | M | 51 | 15.0 | NR | NR | NR |
| 2 | Murakami, 2010 [ | F | 40 | 20.0 | No | T1bN1 | ALK |
| 3 | Noroxe, 2012 [ | M | 50 | 10.0 | Yes | T2aN1 | Wild type |
| 4 | Tomizawa, 2013 [ | M | 43 | 15.0 | No | T2aN0 | ALK |
| 5 | Tsukamoto, 2014 [ | M | 43 | 15.0 | No | T1cN2 | ALK |
| 6 | Al-Bhimani, 2015 [ | M | 41 | 17.0 | Yes | T1N0 | ALK |
| 7 | Ishida, 2015 [ | M | 58 | 19.0 | NR | T2aN0 | ALK |
| 8 | Matsumoto, 2016 [ | M | 58 | 22.0 | Yes | T3N2 | ALK |
| 9 | Zito Marino, 2016 [ | M | 35 | 10.0 | No | T2aN0 | ALK |
| 10 | Sonoda, 2017 [ | M | 61 | 19.0 | NR | T2aN0 | Wild type |
| 11 | Isono, 2018 [ | M | 45 | 11.0 | Yes | T1aN1 | ALK |
| 12 | Sonoda, 2019 [ | F | 61 | 10.1 | No | T1aN1 | Wild type |
| 13 | Sonoda, 2019 [ | F | 70 | 10.1 | No | T1bN1 | Wild type |
| 14 | Sonoda, 2019 [ | M | 70 | 10.3 | Yes | T1bN0 | Wild type |
| 15 | Sonoda, 2019 [ | F | 70 | 10.4 | No | T1aN0 | EGFR exon 19 |
| 16 | Sonoda, 2019 [ | F | 49 | 11.4 | Yes | T2aN0 | Wild type |
| 17 | Sonoda, 2019 [ | M | 58 | 11.6 | Yes | T1bN0 | EGFR exon 21 |
| 18 | Sonoda, 2019 [ | F | 56 | 12.6 | No | T1aN1 | EGFR exon 21 |
| 19 | Sonoda, 2019 [ | F | 69 | 13.0 | No | T1cN1 | EGFR exon 20 |
| 20 | Sonoda, 2019 [ | M | 65 | 13.4 | Yes | T3N0 | Wild type |
| 21 | Sonoda, 2019 [ | M | 50 | 13.8 | Yes | T2aN1 | NR |
| 22 | Sonoda, 2019 [ | F | 49 | 17.8 | No | T2aN0 | ALK |
| 23 | Sonoda, 2019 [ | M | 55 | 19.8 | Yes | T3N0 | ALK |
| 24 | Matsuo, 2020 [ | F | 54 | 16.0 | No | T1cN2 | ALK |
| 25 | Yang, 2021 [ | M | 30 | 11.7 | NR | T2aN0 | KRAS G12D |
| 26 | Park, 2023 [ | F | 56 | 10.5 | No | T3N1 | RET KIF13A |
| 27 | Current case | F | 66 | 10.3 | Yes | T1bN0 | EGFR exon 20 |
| Characteristics | ALK-rearranged patients | EGFR-mutated patients | No EGFR or ALK alteration | Total patients | p-value |
| (N=11) | (N=5) | (N=11) | (N=27) | ||
| Median age (range) | 45.0 (35-58) | 58.0 (56-70) | 51.0 (30-70) | 54.0 (30-70) | 0.03 |
| Histology: | |||||
| -Adenocarcinoma | 11 (100) | 5 (100) | 10 (91) | 26 (96) | 0.47 |
| -Atypical carcinoid | 0 (0) | 0 (0) | 1 (9) | 1 (4) | |
| Sex: | |||||
| -Female | 3 (27) | 4 (80) | 4 (36) | 11 (41) | 0.13 |
| -Male | 8 (73) | 1 (20) | 7 (63) | 16 (59) | |
| Smoking history: | |||||
| -No | 6 (60) | 3 (60) | 3 (38) | 12 (52) | 0.59 |
| -Yes | 4 (40) | 2 (40) | 5 (63) | 11 (48) | |
| Nodal involvement: | |||||
| -No | 7 (64) | 4 (80) | 5 (50) | 16 (62) | 0.52 |
| -Yes | 4 (36) | 1 (20) | 5 (50) | 10 (38) | |
| T stage: | |||||
| -T1 | 5 (45) | 5 (100) | 3 (30) | 13 (50) | 0.04 |
| -T2-T3 | 6 (55) | 0 (0) | 7 (70) | 13 (50) | |
| N stage: | |||||
| -N0 | 7 (64) | 4 (80) | 5 (50) | 16 (62) | 0.02 |
| -N1 | 0 (0) | 1 (20) | 5 (50) | 6 (23) | |
| -N2 | 4 (36) | 0 (0) | 0 (0) | 4 (15) | |
| Stage group: | |||||
| -Stage I | 6 (55) | 4 (80) | 4 (40) | 14 (54) | 0.11 |
| -Stage II | 1 (9) | 1 (20) | 5 (50) | 7 (27) | |
| -Stage III | 4 (36) | 0 (0) | 1 (10) | 5 (19) | |
| Factors | Univariable Hazard Ratio (95% CI) | p-value |
| Age: | ||
| -Per year increase | 1.01 (0.97-1.06) | 0.58 |
| Sex: | ||
| -Female | 1.41 (0.64-3.09) | 0.39 |
| -Male | Reference | |
| Smoking history: | ||
| -Yes | 0.93 (0.40-2.18) | 0.88 |
| -No | Reference | |
| T-stage: | ||
| -T1 | 1.75 (0.78-3.90) | 0.18 |
| -T2 or T3 | Reference | |
| Node positive: | ||
| -Yes | 1.19 (0.52-2.73) | 0.68 |
| -No | Reference | |
| Gene alteration: | ||
| -ALK rearrangement | 0.30 (0.13-0.73) | 0.008 |
| -EGFR mutation, none, unknown | Reference | |
| Stage group: | ||
| -Per stage increase | 0.87 (0.53-1.43) | 0.59 |
| Patient number | Test in initial cancer | Test in recurrent cancer | Presence of pulmonary metastasis | Presence of lesion at surgical site | Presence of extra-thoracic metastasis | Sites of distant metastasis at recurrence |
| 2 | NA | RT-PCR, FISH, IHC | Yes | No | No | Pleura, bilateral lungs |
| 4 | RT-PCR, FISH | RT-PCR, FISH | No | Yes | No | None |
| 5 | RT-PCR, FISH, IHC | RT-PCR, IHC | Yes | No | Yes | Contralateral lung, abdominal lymph node |
| 6 | FISH, IHC | FISH, IHC | No | No | No | Pleura |
| 7 | FISH, IHC | FISH, IHC | Yes | No | No | Bilateral lungs |
| 8 | IHC | FISH | No | No | No | Chest wall, sternum |
| 9 | FISH, IHC | NA | No | Yes | No | None |
| 11 | IHC | IHC | No | Yes | Yes | Pleura, mediastinal and supraclavicular node |
| 22 | IHC | IHC | Yes | No | No | Ipsilateral lung |
| 23* | IHC | IHC | No | No | No | None |
| 24 | RT-PCR, IHC | RT-PCR, IHC | No | No | Yes | Brain, liver |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Lung Cancer Diagnosis and Treatment · Lung Cancer Research Studies
Introduction
Following curative surgery, patients with early-stage non-small cell lung cancer (NSCLC) still face a risk of recurrent disease. This risk typically increases along with the cancer stage. For example, in a study of 1619 patients with stage I to III NSCLC, recurrences occurred in 22% of stage I patients, 33% among stage II patients, and 40% among stage III patients [1]. Most recurrences occurred within the first two years after surgery and higher stages predicted earlier recurrence. For instance, in stage II and III lung cancers, 80% of all recurrences occurred within two years, compared with only 60% among stage I. However, regardless of stage, almost all recurrences can be expected to have occurred by five years after surgery. Currently, the national guideline recommends surveillance imaging for the first five years after definitive treatment followed by optional yearly surveillance thereafter [2].
Late recurrence, defined as beyond five years after surgery as well as ultra-late recurrence, defined as beyond 10 years after surgery, have been rarely investigated in NSCLC. In a study of 517 patients with stage IA NSCLC, there were 22 patients (4.8%) who could be considered as having a late recurrence, with the greatest time to recurrence being 113 months [3]. Ultra-late recurrence is even less commonly reported. In a study from Japan containing 1458 resected NSCLC patients, 12 patients (2.5%) developed recurrence later than 10 years after surgery [4]. A study of late and ultra-late recurrence NSCLC can be challenging due to the needed prolonged follow-up time as well as the difficulty in differentiating between recurrent and new primary lung cancer. The criteria proposed by Martini and Melamed which are based on histological similarity, mediastinal lymph node involvement, and a two-year disease-free interval, can be helpful [5]. In addition, genetic alteration can also be used to confirm that both initial and recurrent cancers share the same clonal origin.
To date, there is still a paucity of literature on ultra-late recurrence in NSCLC. The topic of ultra-late recurrence is clinically relevant because it may have an implication on the duration and extent of surveillance follow-up. In this article, we report on a patient who developed ultra-late recurrence, presenting as brain metastasis after over 10 years from resection. The tissue specimens from both the initial resection of stage IA lung cancer and the resection of brain metastasis were compared. The same clonality was confirmed based on the presence of epidermal growth factor receptor (EGFR) exon 20 insertion in both specimens. We also performed a literature review and conducted a pooled analysis to identify factors associated with time to recurrence among NSCLC cases developing ultra-late recurrence.
Case presentation
A 66-year-old female patient with a past medical history of cervical cancer, breast cancer, and a 30-pack-year smoking history presented with progressive headaches. Over 10 years ago, a left lower lobectomy was performed for stage T1bN0M0, IA2, well-differentiated adenocarcinoma. Originally, the mass in the left lower lobe was detected during a surveillance computer tomography (CT) scan indicated for the patient's 30-year history of smoking. The patient received no adjuvant chemotherapy. At presentation, a magnetic resonance imaging (MRI) of the brain revealed a solitary 1 cm lesion in the right frontal lobe as well as an enhancement suggesting leptomeningeal involvement (Figure 1). Cerebrospinal fluid examination revealed atypical cells highly suspicious for malignancy. Computerized and positron emission tomography demonstrated no extracranial disease.
Magnetic resonance imaging T1 axial image of brain
The repeated head MRI with and without contrast demonstrated metastatic disease with new parenchymal and leptomeningeal deposits. The patient underwent right frontal stereotactic craniotomy with tractography under stereotactic guidance and Ommaya insertion, followed by whole-brain radiation. Pathological examination showed adenocarcinoma of the lung, positive for thyroid transcription factor 1 and CK7 and negative for CK20, GATA3, mammaglobin, CDX2, and mutant BRAF-V600E. Mismatch repair protein expression was retained (MLH1, PMS2, MSH2, MSH6). A targeted next-generation sequencing analysis revealed an in-frame EGFR exon 20 insertion. We retrieved the specimen from initial lung surgery 10 years ago for comparison. The histology was similar, and EGFR exon 20 insertion was also identified.
At the time of this report, 10 months after surgery, the patient continued to receive intrathecal topotecan with stable disease.
Discussion
Literature review and pooled analysis
We performed a literature search on MEDLINE Pubmed and Google Scholar published from January 2010 to 2023 for late or ultra-late recurrence in NSCLC. The reference list of each retrieved article was checked for additional publications. Ultra-late recurrence was defined as the time between the initial surgery and the first recurrence of ≥10 years. Abstracts and full reports were reviewed to extract patient and cancer characteristics including EGFR or anaplastic lymphoma kinase (ALK) alterations. For uniformity of analysis, tumor sizes and stages were converted into the American Joint Committee on Cancer Staging 8th edition [6], when feasible. A pooled analysis was conducted with the outcome of interest being time to recurrence defined as time from initial surgery to the ultra-late recurrence. Descriptive statistics, including median and range, were used for continuous variables as well as percentage and count, for categorical variables. Non-parametric Mann-Whitney U-test was used to compare age. Pearson Chi-square or Fisher exact test was used to compare categorical variables. Median time to recurrence was estimated by the method of Kaplan-Meier and the log-rank test was used to compare groups. Multivariable analysis was performed using Cox Proportional Hazard models. Variable selection was performed using backward stepwise elimination method with a significant level to stay set at 0.10. All p-values were 2-tailed and significance level was set at <0.05. Analyses and graphics were performed on SPSS version 28 (IBM, Armonk, NY, USA).
Results
Publication and Patient Characteristics
Our literature search identified 16 publications describing 27 cases with ultra-late recurrence, including the case described in this report (Table 1). Most publications emanated from institutions in Japan, contributing to 21 patients. The remaining publications were from institutions in Canada, Italy, Denmark, Korea, and the United States. The largest report was published in 2019, containing 12 cases.
Patient characteristics were obtained from 27 patients (Table 2). There were five patients with EGFR mutation, 11 patients with ALK rearrangement, and 11 patients with no EGFR or ALK alterations or unknown biomarker status. Among those without EGFR or ALK alterations, one patient had a KRAS mutation, and one patient had a RET rearrangement. Overall, the median age of patients was 54 years (range 30-70 years). All of those with molecular alterations had both specimens from resection and specimens from recurrence examined to confirm biomarker similarity except for patient number 2 due to the degradation of initial tissue and patient number 9 due to the inadequate biopsy sample in the recurrence cancer. Patient number 9 did achieve a partial tumor response to ALK inhibitor treatment to further substantiate the presence of ALK rearrangement.
Table 2: Characteristic of patients and initial tumor by EGFR/ALK statusValues for characteristics are median (IQR) or N (%). A p-value <0.05 was considered statistically significant.EFGR = epidermal growth factor receptor; ALK = anaplastic lymphoma kinase; IQR = interquartile range
Patients with ALK rearrangement were younger than those of patients with EGFR mutation or with no ALK/EGFR alteration: 49 years compared with 58 and 61 years, respectively (p=0.001). The oldest patient with ALK rearrangement was 58 years while the oldest patient in this series was 70 years. No significant difference was found in terms of sex, smoking history, or nodal involvement. There was a statistically higher proportion of patients with N-2 disease among those with ALK rearrangement.
Ultra-Late Recurrence
Time to recurrence was analyzed among 27 patients. The median time to recurrence was 13.4 years (95% CI: 11.4-15.4 months). Patients with ALK rearrangement had a significantly longer time to recurrence than other groups of patients, with a median of 17.0 years (95% CI: 13.9-20.0) compared with 11.6 years (95% CI: 9.3-13.9) among those with EGFR mutation and 11.7 years (95% CI: 8.4-15.0) among those without EGFR or ALK alteration, p=0.004 (Figure 2).
Time to recurrence by EGFR/ALK statusEFGR = epidermal growth factor receptor; ALK = anaplastic lymphoma kinase
We performed univariable and multivariable analyses considering biomarkers, sex, age, smoking status, nodal involvement, T stage, and stage group (Table 3). Only ALK rearrangement was found to be an independent predictor of delayed time to recurrence, with a hazard ratio of 0.30 (95% CI: 0.13-0.73, p=0.008). Finally, we reviewed the pattern of recurrence among patients with ALK rearrangement (Table 4). In all patients, the recurrence could be visualized by routine computerized tomography of the chest including the upper abdomen.
Table 3: Factors associated with time to recurrenceValues are univariable hazard ratios (95% CI). A p-value <0.05 was considered statistically significant.CI = confidence interval; EFGR = epidermal growth factor receptor; ALK = anaplastic lymphoma kinase
Discussion
In this article, we reported a case of ultra-late recurrence adenocarcinoma with EGFR exon 20 insertion. To our knowledge, only four previous cases of ultra-late recurrence with EGFR mutation have been reported in the literature. Nonetheless, our literature review showed that there are many more cases of ultra-late recurrence with ALK rearrangement. A pooled analysis of reported cases demonstrated that ALK rearrangement was associated with a longer time to recurrence than EGFR mutation or no ALK/EGFR alterations.
To our knowledge, the current report contains the largest number of patients with ultra-late recurrence and is the first to explore potential factors associated with the phenomenon. In pulmonary adenocarcinoma, EGFR mutation is generally more common than ALK rearrangement. Specifically, while EGFR mutation is present ranging from 15% in Western countries to 50% in Asian countries, ALK rearrangement is present in only 5-10% of patients [21]. On the contrary, we found that among NSCLC with ultra-late recurrence, there were more cases of ALK rearrangement than EGFR mutation. This finding may be explained, in part, by the fact that patients with ALK rearrangement are generally younger than those with EGFR mutation, thus longer life expectancy to allow for a longer observation period for recurrence. However, age alone was unlikely to be the single explanation, given a much larger pool of patients without ALK rearrangement and the fact that age was not found to be a significant predictor of time to recurrence in this small study.
Very little research has been conducted for ultra-late recurrence in NSCLC; however, in breast cancer, ultra-late recurrence has been associated with tumors with positive estrogen receptor (ER) status. The recurrence risk of ER-positive breast cancer following surgery is initially lower than ER-negative disease; however, it will surpass the risk among ER-negative cancer after about eight years after surgery and will persist for up to 25 years [22]. Some authors have proposed that late recurrence is the result of metastatic cancer becoming dormant and later being reactivated as patients age [23]. However, it remains unknown what causes cancer cells to become dormant. There is no evidence to suggest that EGFR or ALK-positive adenocarcinomas of the lung have a slower growth rate compared to other lung cancers. In previous studies of resected early-stage NSCLC, recurrence during five to 10 years after surgery has been associated with factors such as race, histology, and vascular invasion [1,3]. Unfortunately, no information on EGFR or ALK was available.
Our study suggests a unique biological characteristic of ALK-rearranged lung cancer in its association with ultra-late recurrence. Nonetheless, some limitations should be noted. As this work is based largely on published studies, it can suffer from reporting and publication bias. However, the bias should be equally present for both EGFR and ALK cancers, thus minimizing its impact on the statistical comparison. Another consideration is that most reported cases are from Asian centers, and this may limit its generalizability.
Conclusions
In summary, among NSCLC cases with ultra-late recurrence, ALK rearrangement is prevalent and ALK rearrangement is associated with greater time to recurrence than EGFR mutation. Given the potential implication for long-term follow-up need among patients with ALK rearrangement, it may be advisable to check resected early-stage lung cancer for ALK rearrangement especially among younger patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Timing, sites, and correlates of lung cancer recurrence Clin Lung Cancer Karacz CM Yan J Zhu H Gerber DE 1271352120203193221610.1016/j.cllc.2019.12.001PMC 7061059 · doi ↗ · pubmed ↗
- 2NCCN Guidelines® Insights: non-small cell lung cancer, version 2.2023 J Natl Compr Canc Netw Ettinger DS Wood DE Aisner DL 340350212023 https://pubmed.ncbi.nlm.nih.gov/37015337/3701533710.6004/jnccn.2023.0020 · doi ↗ · pubmed ↗
- 3Long-term outcome and late recurrence in patients with completely resected stage IA non-small cell lung cancer J Thorac Oncol Maeda R Yoshida J Ishii G 12461250520102055915210.1097/JTO.0b 013e 3181 e 2f 247 · doi ↗ · pubmed ↗
- 4Ultra-late recurrence of non-small cell lung cancer over 10 years after curative resection Cancer Manag Res Sonoda D Matsuura Y Ichinose J 676567741120193141006510.2147/CMAR.S 213553 PMC 6648654 · doi ↗ · pubmed ↗
- 5Incidence of local recurrence and second primary tumors in resected stage I lung cancer J Thorac Cardiovasc Surg Martini N Bains MS Burt ME 1201291091995781578710.1016/S 0022-5223(95)70427-2 · doi ↗ · pubmed ↗
- 6The IASLC lung cancer staging project: external validation of the revision of the TNM stage groupings in the eighth edition of the TNM classification of lung cancer J Thorac Oncol Chansky K Detterbeck FC Nicholson AG 110911211220172846125710.1016/j.jtho.2017.04.011 · doi ↗ · pubmed ↗
- 7Spinal metastasis from lung cancer fifteen years after surgery presenting a pseudohemangioma appearance of the vertebra: a case report Spine (Phila Pa 1976) Inaoka T Takahashi K Aburano T Miyokawa N Tandai S Kobayashi T Matsuno T 0935201010.1097/BRS.0b 013e 3181 aa 21d 520075786 · doi ↗ · pubmed ↗
- 8Recurrent EML 4-ALK-associated lung adenocarcinoma with a slow clinical course Lung Cancer Murakami S Yokose T Saito H 3613646920102065962010.1016/j.lungcan.2010.05.019 · doi ↗ · pubmed ↗