Association Between Treated Periodontal Disease and Febrile Neutropenia in Perioperative Chemotherapy for Breast Cancer: A Retrospective Cohort Study
Ai Yamaguchi, Yuki Kataoka, Kazuma Fujimura, Tomoe Taji, Hirofumi Suwa

TL;DR
This study found no significant increase in febrile neutropenia in breast cancer patients with treated periodontal disease during chemotherapy.
Contribution
The study provides evidence that prior dental treatment for periodontal disease does not increase febrile neutropenia risk during breast cancer chemotherapy.
Findings
FN incidence was 36.4% in the periodontal group and 25.9% in the control group.
The adjusted odds ratio for FN incidence was 1.52, but it was not statistically significant.
Abstract
Background: This study aimed to examine whether the incidence of febrile neutropenia (FN) during perioperative chemotherapy for breast cancer increased in patients with periodontal disease who had received prior dental treatment. Methods: This retrospective cohort study conducted at a single tertiary care center included patients diagnosed with clinical stages I-III of breast cancer and had started neoadjuvant or adjuvant intravenous chemotherapy between July 2015 and November 2021. The exposure was periodontal disease (probing depth ≥6 mm) diagnosed by dentists before the start of chemotherapy. Almost all the patients received dental treatment and oral care before initiating chemotherapy. The primary outcome was FN incidence during chemotherapy. We used a multivariable logistic regression model adjusted for age, diabetes mellitus, chemotherapy regimen, and the mean relative dose…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
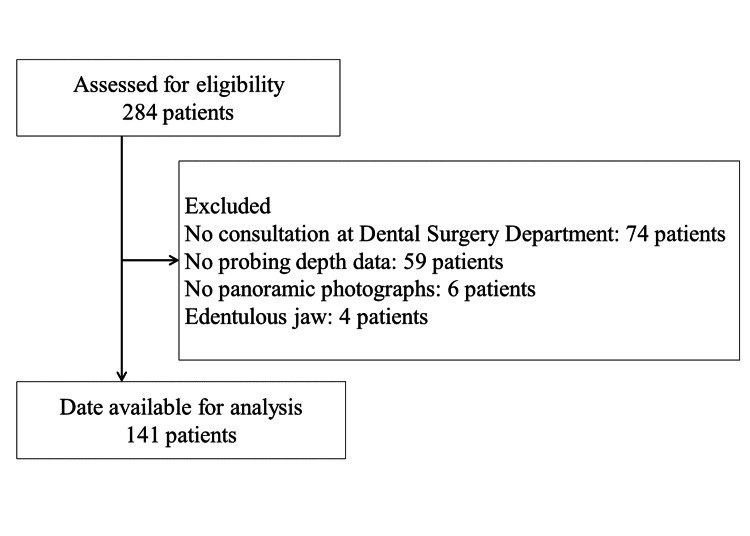 Figure 1
Figure 1| Variable | All patients (N =141) | Probing depth (mm) | |
| ≥ 6 (N =33) | < 6 (N =108) | ||
| Age, median (range) | 55 (25-77) | 61 (41-77) | 54 (25-76) |
| Postmenopausal, n (%) | 85 (60.3) | 24 (72.7) | 61 (56.5) |
| Histology, n (%) | |||
| Invasive ductal | 130 (92.2) | 30 (90.9) | 100 (92.6) |
| Invasive lobular | 4 (2.8) | 1 (3.0) | 3 (2.8) |
| Other | 5 (3.5) | 2 (6.1) | 3 (2.8) |
| Missing data | 2 (1.4) | 0 (0) | 2 (1.9) |
| Histological grade, n (%) | |||
| Grade 1 | 28 (19.9) | 7 (21.2) | 21 (19.4) |
| Grade 2 | 87 (61.7) | 20 (60.6) | 67 (62.0) |
| Grade 3 | 21 (14.9) | 3 (9.1) | 18 (16.7) |
| Missing data | 5 (3.5) | 3 (9.1) | 2 (1.9) |
| Clinical stage, n (%) | |||
| Stage 1 | 31 (22.0) | 12 (36.4) | 19 (17.6) |
| Stage 2 | 86 (61.0) | 16 (48.5) | 70 (64.8) |
| Stage 3 | 22 (15.6) | 4 (12.1) | 18 (16.7) |
| Missing data | 2 (1.4) | 1 (3.0) | 1 (0.9) |
| ER positive, n (%) | 85 (60.3) | 20 (60.6) | 65 (60.2) |
| PR positive, n (%) | 74 (52.5) | 16 (48.5) | 58 (53.7) |
| HER2 positive, n (%) | 45 (31.9) | 11 (33.3) | 34 (31.5) |
| NAC, n (%) | 57 (40.4) | 11 (33.3) | 46 (42.6) |
| Chemotherapy regimen, n (%) | |||
| Taxane plus anthracycline-based | 108 (76.6) | 25 (75.8) | 83 (76.9) |
| EC or AC or FEC → DTX or PTX or Nab-PTX | 96 (68.1) | 21 (63.6) | 75 (69.4) |
| Dose-dense therapy | 12 (8.5) | 4 (12.1) | 8 (7.4) |
| Non-anthracycline-based | 31 (22.0) | 8 (24.2) | 23 (21.3) |
| TC | 16 (11.3) | 1 (3.0) | 15 (13.9) |
| TCb | 4 (2.8) | 1 (3.0) | 3 (2.8) |
| DTX | 1 (0.7) | 0 (0) | 1 (0.9) |
| Nab-PTX | 2 (1.4) | 1 (3.0) | 1 (0.9) |
| PTX | 8 (5.7) | 5 (15.2) | 3 (2.8) |
| Other | 2 (1.4) | 0 (0) | 2 (1.9) |
| Tra or/plus Per | 45 (31.9) | 11 (33.3) | 34 (31.5) |
| G-CSF for prophylaxis, n (%) | 46 (32.6) | 12 (36.4) | 34 (31.5) |
| HbA1c ≥ 6.5%, n (%) | 14 (9.9) | 6 (18.2) | 8 (7.4) |
| Hypertension, n (%) | 27 (19.1) | 11 (33.3) | 16 (14.8) |
| Hyperlipidemia, n (%) | 26 (18.4) | 7 (21.2) | 19 (17.6) |
| Asthma, n (%) | 5 (3.5) | 1 (3.0) | 4 (3.7) |
| Hypothyroidism, n (%) | 4 (2.8) | 3 (9.1) | 1 (0.9) |
| Atrial fibrillation, n (%) | 3 (2.1) | 0 (0) | 3 (2.8) |
| Hyperthyroidism, n (%) | 2 (1.4) | 1 (3.0) | 1 (0.9) |
| Other comorbidities, n (%) | 7 (5.0) | 1 (3.0) | 6 (5.6) |
| Assessment of periodontal condition as per the community periodontal index | |||
| Bleeding on probing, n (%) | 41 (29.1) | 15 (45.5) | 26 (24.1) |
| Dental calculus, n (%) | 81 (57.4) | 16 (48.5) | 65 (60.2) |
| Number of teeth, median (range) | 27 (5-32) | 27 (11-32) | 27 (5-32) |
| Tooth mobility, n (%) | 11 (7.8) | 4 (12.1) | 7 (6.5) |
| Periapical lesion, n (%) | 21 (14.9) | 7 (21.2) | 14 (13.0) |
| RABL ≥ Stage Ⅲ, n (%) | 34 (24.1) | 17 (51.5) | 17 (15.7) |
| Number of oral care visits per month, median (range) | 1.1 (0-3.4) | 1.1 (0-2.3) | 1.1 (0-3.4) |
| Variable | All patients (N =141) | Probing depth (mm) | ||
| ≥ 6 (N =33) | < 6 (N =108) | |||
| FN, n (%) | 40 (28.4) | 12 (36.4) | 28 (25.9) | |
| Hospital visit at the time of FN, n (%) | 8 (5.6) | 2 (6.0) | 6 (5.6) | |
| Hospitalization due to FN, n (%) | 5 (3.6) | 1 (3.0) | 4 (3.7) | |
| Adverse events, n (%) | ||||
| Neutropenia | Grade 2 | 9 (6.4) | 4 (12.1) | 5 (4.6) |
| ≥ Grade 3 | 106 (75.2) | 23 (69.7) | 83 (76.9) | |
| Anemia | Grade 2 | 51 (36.2) | 12 (36.4) | 39 (36.1) |
| ≥ Grade 3 | 6 (4.3) | 1 (3.0) | 5 (4.6) | |
| Platelet count decrease | Grade 2 | 4 (2.8) | 1 (3.0) | 3 (2.8) |
| ≥ Grade 3 | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| AST increased | Grade 2 | 1 (0.7) | 0 (0.0) | 1 (0.9) |
| ≥ Grade 3 | 4 (2.8) | 0 (0.0) | 4 (3.7) | |
| ALT increased | Grade 2 | 15 (10.6) | 4 (12.1) | 11 (10.2) |
| ≥ Grade 3 | 11 (7.8) | 1 (3.0) | 10 (9.3) | |
| Delayed days, median (range) | 7 (0-56) | 5 (0-56) | 7 (0-56) | |
| Delayed days (≥ 15 days), n (%) | 29 (20.6) | 3 (9.1) | 26 (24.1) | |
| RDI%, median (range) | 94.2 (51.6-101.8) | 96.1 (51.6-100.3) | 94.2 (52.8-101.8) | |
| RDI (< 85%), n (%) | 25 (17.7) | 6 (18.2) | 19 (17.6) | |
| Variable | Univariate analysis | ||
| OR (95% CI) | P-value | ||
| Age | 1.01 (0.97-1.04) | 0.56 | |
| Taxane plus anthracycline-based | No | 1.00 | |
| Yes | 2.68 (0.95-7.55) | 0.061 | |
| Non-anthracycline-based | No | 1.00 | |
| Yes | 0.21 (0.06-0.74) | 0.015 | |
| G-CSF for prophylaxis | No | 1.00 | |
| Yes | 0.41 (0.17-0.99) | 0.048 | |
| RDI | ≥ 85% | 1.00 | |
| < 85% | 0.57 (0.20-1.67) | 0.31 | |
| Neutropenia | < Grade 3 | 1.00 | |
| ≥ Grade 3 | 5.72 (1.64-19.9) | 0.006 | |
| HbA1c | < 6.5% | 1.00 | |
| ≥ 6.5% | 1.46 (0.45-4.66) | 0.52 | |
| Probing depth | < 6 mm | 1.00 | |
| ≥ 6 mm | 1.63 (0.71-3.74) | 0.24 | |
| Bleeding on probing | No | 1.00 | |
| Yes | 1.26 (0.56-2.77) | 0.57 | |
| Dental calculus | No | 1.00 | |
| Yes | 2.11 (0.96-4.61) | 0.06 | |
| Number of teeth | 0.98 (0.92-1.06) | 0.75 | |
| Tooth mobility | No | 1.00 | |
| Yes | 1.49 (0.41-5.40) | 0.54 | |
| Periapical lesion | No | 1.00 | |
| Yes | 0.75 (0.25-2.23) | 0.61 | |
| Variable | Multivariate analysis | ||||
| Model 1 | Model 2 | ||||
| OR (95% CI) | P-value | OR (95% CI) | P-value | ||
| Age | 1.00 (0.97-1.04) | 0.80 | 1.01 (0.97-1.05) | 0.42 | |
| Non-anthracycline-based | No | 1.00 | |||
| Yes | 0.20 (0.05-0.71) | 0.013 | |||
| RDI | ≥ 85% | 1.00 | |||
| < 85% | 0.53 (0.17-1.65) | 0.217 | |||
| HbA1c | < 6.5% | 1.00 | 1.00 | ||
| ≥ 6.5% | 1.30 (0.39-4.27) | 0.66 | 1.30 (0.38-4.42) | 0.67 | |
| Probing depth | < 6 mm | 1.00 | 1.00 | ||
| ≥ 6 mm | 1.54 (0.65-3.67) | 0.32 | 1.52 (0.62-3.73) | 0.36 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral health in cancer treatment · Oral Health Pathology and Treatment · Neutropenia and Cancer Infections
Introduction
Periodontal disease not only causes tooth loss but also has systemic effects. It is a risk factor for pneumonia [1], and it could affect the prognosis of diabetes negatively [2]. The Community Periodontal Index (CPI) is a screening method for assessing periodontal status, which uses the World Health Organization (WHO) probe to evaluate periodontal pockets, gingival bleeding, and calculus [3]. The prevalence of periodontal disease is quite high. In the Japanese general population, the proportion of individuals with periodontal pockets ≥4 mm in depth increased with age, with approximately 45% and 60% of the individuals in their 40s and 60s, respectively. The proportion of those with gingival bleeding was >30% among individuals aged ≥15 years and >40% in those aged 30-55 years [4].
Moreover, gingivitis and periodontitis are a concern in patients with neutropenia undergoing chemotherapy. Microorganisms can migrate from the ulcerated periodontal pocket epithelium into the bloodstream [5]. Bacterial products, such as lipopolysaccharides, and pro-inflammatory cytokines in the inflamed and infected periodontal lesions may induce a cascade of systemic inflammatory responses [6,7]. In fact, a retrospective study of hospitalized adults with leukemia demonstrated that patients with gingivitis/periodontitis had a higher risk of sepsis (27.8% vs. 19.6%), bacterial infections (19.5% vs. 10.1%), and fungal infections (20.7% vs. 10.7%) than those without [8]. However, to date, no studies on solid tumors have been reported, which are usually treated with less intense myelosuppressive chemotherapy than hematopoietic malignancies.
This study examined whether the incidence of febrile neutropenia (FN) increases in patients with periodontal disease during perioperative chemotherapy for breast cancer.
Materials and methods
Study design
This retrospective cohort study was conducted at a single tertiary care center. It was approved by the Ethics Committee of our institution (2-144) and was conducted in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki). The duration of the study is from November 2020 to May 2022. Complete information about the study was made available to the participants, who were given the opportunity to refuse participation.
We identified patients for this study using chemotherapy databases and retrieved their clinical information, including clinical findings, dental records, chemotherapy regimen, tumor type, and toxicity data, from the hospital’s electronic medical records. The STROBE checklist [9] followed is provided as an online resource [10].
Participants
The inclusion criteria for this study were age ≥20 years, histological diagnosis of invasive breast cancer clinical stages I-III according to the Union for International Cancer Control [11], and start of neoadjuvant or adjuvant intravenous chemotherapy between July 2015 and November 2021. Patients who had not consulted our Dental Surgery Department before chemotherapy, those without probing depth data during dental examination, and those with edentulous jaws were excluded.
Chemotherapy regimens
The chemotherapy regimen was determined according to the Japanese Breast Cancer Society Clinical Practice Guidelines [12]. The regimen was selected at the discretion of the clinician if there were concerns regarding toxicity or contraindications to a particular drug. Most cases received sequential administration of four cycles of epirubicin 90 mg/m^2^ plus cyclophosphamide 600 mg/m^2^ (EC) every 21 days and four cycles of docetaxel (DTX) 75 mg/m^2^ every 21 days (or 12 cycles of paclitaxel [PTX] 80 mg/m^2^ every seven days). In human epidermal growth factor receptor type 2-positive cases, trastuzumab or trastuzumab plus pertuzumab was administered concurrently with taxane. Granulocyte colony-stimulating factor (G-CSF) was administered prophylactically with four to six cycles of DTX 75 mg/m^2^ plus cyclophosphamide 600 mg/m^2^ every 21 days (TC) and dose-dense chemotherapy (four cycles of EC every 14 days administered sequentially with four cycles of PTX 175 mg/m^2^ every 14 days or 12 cycles of PTX 80 mg/m^2^ every seven days). G-CSF was administered in other regimens at the discretion of the clinician. There was no concomitant use of other therapies during intravenous chemotherapy.
Exposure
The exposure was periodontal disease, and the presence or absence of the exposure was assessed by dentists before starting chemotherapy. The probing depth around all the teeth was evaluated using the WHO probe. It was defined as the distance from the gingival margin to the base of the pocket and expressed in millimeters; periodontal disease was defined when the probing depth was ≥6 mm, according to the CPI recommended by the WHO [3].
The radiographic alveolar bone loss was evaluated by a dentist using panoramic radiography to determine whether it extended to the middle or apical third of the root (≥Stage III according to the American Academy of Periodontology and the European Federation of Periodontology staging system [13]).
Based on complete or partial pre-cancer chemotherapy dental treatment protocols [14], personalized dental treatment was administered before starting chemotherapy. Routine oral care was provided during chemotherapy, including dental scaling, professional tooth cleaning, extraction of infected teeth, and tooth brushing instructions.
Primary outcome
The primary outcome was the incidence of FN during intravenous chemotherapy. The observation period was defined as that from the start to the end of chemotherapy.
The onset of FN was defined as antibiotic administration at some point between the day after starting chemotherapy and the last day of chemotherapy. Antibiotics were limited to those used for FN at our institution, i.e., ciprofloxacin, amoxicillin-clavulanate, levofloxacin, meropenem, cefepime, piperacillin, tazobactam, and vancomycin. We excluded patients with no episodes of axillary temperature ≥37.5°C documented in the medical records before or after the date of antibiotic administration.
As a countermeasure against FN, oral antibiotics (ciprofloxacin plus amoxicillin-clavulanate or levofloxacin) were administered at the start of chemotherapy. We instructed patients to take oral antibiotics without visiting our institution if they recorded an axillary temperature ≥37.5°C after the start of chemotherapy. If the patient was asymptomatic and the fever resolved within a few days of receiving oral antibiotics, there was no need to visit our institution.
Secondary outcome
The secondary outcomes were a mean relative dose intensity (RDI) <85%, percentage of delayed days for chemotherapy (≥15 days), and incidence of hematologic adverse events ≥Grade 2 according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 5.0. The RDI was calculated as follows: (actual dose [mg/m^2^/week] / standard dose [mg/m^2^/week]) × 100 [15].
Statistical analysis
Univariate and multivariate analyses were performed using logistic regression to determine the odds ratio (OR) and 95% confidence interval (CI). The confounders considered were age, diabetes, chemotherapy regimen, and the RDI. Model 1 was adjusted for age, diabetes mellitus (glycated hemoglobin [HbA1c] ≥6.5% or <6.5%), and probing depth (≥6 mm or <6 mm). Model 2 was adjusted for age, diabetes mellitus (HbA1c ≥6.5% or <6.5%), probing depth (≥6 mm or <6 mm), non-anthracycline-based chemotherapy regimen (yes or no), and RDI (<85% or ≥85%). Two-sided probability testing was used; P-values <0.05 were considered statistically significant. Statistical analyses were performed using EZR 1.55 software package (R statistical software version 4.1.2, R Foundation for Statistical Computing, Vienna, Austria) [16].
Results
In total, 141 patients were included in the analysis (Figure 1). The observation period lasted until May 15, 2022, when all patients in the study had completed chemotherapy. There were no dropouts during the observation period. Baseline patient performance status was 0 or 1, absolute neutrophil count ≥1500/µL, total bilirubin <2 mg/dL, aspartate aminotransferase (AST) <100 U/L, alanine aminotransferase (ALT) <100 U/L, and creatinine <1.5 mg/dL. (Only one patient had an ALT of 138 U/L and received a reduced dose.) Table 1 shows the baseline clinicopathological characteristics of the patients.
Patient flow chart
The patients were divided into the periodontal group (probing depth ≥6 mm; n = 33) and the control group (probing depth <6 mm; n = 108), and the mean age was greater in the former than in the latter. The number of participants receiving PTX monotherapy was more in the periodontal group than in the control group. Table 2 presents the adverse events, delayed days, and mean RDI values of the two groups.
The incidence of FN was 36.4% (12/33) in the periodontal group and 25.9% (28/108) in the control group. Eight patients had a hospital visit at the time of FN, and blood cultures were collected and confirmed negative in seven patients. The crude OR for FN incidence was 1.63 (95% CI, 0.71-3.74; P = 0.24) (Table 3), and the adjusted OR was 1.52 (95% CI, 0.62-3.73; P = 0.36) (Model 2 in Table 4).
Discussion
This study compared the incidence of FN during perioperative breast cancer chemotherapy between patients with and without periodontal disease. The incidence of FN was slightly higher in the periodontal group than in the control group; however, the confidence interval for the OR straddled unity.
The risk of infection might increase due to chemotherapy-induced neutropenia, particularly in patients with periodontal disease [8,17-21]. Several studies have demonstrated the benefits of dental and periodontal treatments prior to chemotherapy. In patients with hematopoietic malignancies, dental treatment decreases the incidence of systemic infections and inflammatory complications during chemotherapy [22-24]. Almost all patients in this study received dental treatment prior to chemotherapy and oral care during chemotherapy. The risk of FN in patients with or without periodontal disease may be lesser in those who receive dental treatment and oral care than in those who do not.
The risk of FN may be relatively low in patients with periodontal disease who undergo dental treatment. The OR is not high enough to have clinical effects as compared to that of other factors for FN reported previously (TC therapy: OR, 2.67; age ≥65 years: OR, 2.24) [25]. Furthermore, the reported OR was 2.4, assuming a 30% incidence of FN in those with periodontal disease and 15% in those without periodontal disease [8,25]. This suggests that with dental care before or during chemotherapy, the development of FN in patients with periodontal disease does not have clinical effects, and patients can safely undergo chemotherapy.
The strength of this study is its novelty, as we compared the incidence of FN during chemotherapy for solid tumors in patients with and without periodontal disease; however, it has several limitations. First, it was a single-center, retrospective, observational study and may have been underpowered to detect statistically significant differences. Second, cases other than those of FN may have been included because FN was defined when antimicrobials were administered for fever, and assessing the neutrophil count was not mandatory. Third, 74 patients who did not visit the Dental Surgery Department before chemotherapy were excluded, which may have caused a bias in the results. Since dental examinations may not have been performed due to the absence of apparent dental problems, patients with periodontal disease were less likely to be excluded. Therefore, a multicenter prospective study in which all breast cancer patients undergo probing depth measurements before perioperative chemotherapy is warranted.
Conclusions
It was suggested that the risk of FN is relatively low in patients with periodontal disease. FN incidence is not a major concern during perioperative chemotherapy in early breast cancer patients with periodontal disease if they receive regular oral care and dental treatment. The study may be underpowered to detect statistically significant differences. A prospective multicenter study is needed to evaluate the association between periodontal disease and FN in breast cancer patients undergoing preoperative chemotherapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Systematic review of the association between respiratory diseases and oral health J Periodontol Azarpazhooh A Leake JL 146514827720061694502210.1902/jop.2006.060010 · doi ↗ · pubmed ↗
- 2Effect of periodontal disease on diabetes: systematic review of epidemiologic observational evidence J Periodontol Borgnakke WS Ylöstalo PV Taylor GW Genco RJ 05284201310.1902/jop.2013.134001323631574 · doi ↗ · pubmed ↗
- 3Oral Health Surveys: Basic Methods Geneva World Health Organization 2013 https://books.google.co.jp/books?hl=ja&lr=lang_ja|lang_en&id=8r EXDAAAQBAJ&oi=fnd&pg=PP 1&dq=Oral+Health+Surveys:+basic+methods&ots=f EDES 0y C 2r&sig=Y-1Ij M Bs Lhp EMEG Ts_Zz Hn BB 2GU#v=onepage&q=Oral%20Health%20Surveys%3A%20basic%20methods&f=false
- 4Dental diseases survey 11 2023 2016 http://www.mhlw.go.jp/toukei/list/dl/62-28-02.pdf
- 5Actinobacillus actinomycetemcomitans and Porphyromonas gingivalis in nonoral infections Periodontol 2000 van Winkelhoff AJ Slots J 1221352019991052222510.1111/j.1600-0757.1999.tb 00160.x · doi ↗ · pubmed ↗
- 6A systematic review and meta-analyses on C-reactive protein in relation to periodontitis J Clin Periodontol Paraskevas S Huizinga JD Loos BG 2772903520081829423110.1111/j.1600-051X.2007.01173.x · doi ↗ · pubmed ↗
- 7Effect of periodontal treatment on peak serum levels of inflammatory markers Clin Oral Investig Almaghlouth AA Cionca N Cancela JA Décaillet F Courvoisier DS Giannopoulou C Mombelli A 2113212118201410.1007/s 00784-014-1187-424452825 · doi ↗ · pubmed ↗
- 8Poor oral health linked with increased risk of infectious complications in adults with leukemia J Mass Dent Soc Allareddy V Prakasam S Allareddy V 384264201526727815 · pubmed ↗