Diagnostic considerations in the clinical management of sudden swelling of the knee: a case report and review of the literature
Eduard Pavelić, David Glavaš Weinberger, Martin Čemerin, Eduard Rod, Dragan Primorac

TL;DR
This case report discusses the diagnostic challenges of sudden knee swelling in a patient with a history of coronavirus disease 2019 and Clostridium difficile infection.
Contribution
The novelty lies in highlighting the rare co-occurrence of reactive arthritis after coronavirus disease 2019 and Clostridium difficile infection, emphasizing diagnostic considerations.
Findings
The patient's symptoms improved after treating Clostridium difficile infection, despite initial suspicion of septic arthritis.
Human leukocyte antigen B27 positivity was identified, linking to predisposition for reactive arthritis.
Diagnostic challenges in distinguishing septic and reactive arthritis are emphasized, especially in the context of recent coronavirus disease 2019.
Abstract
Reactive arthritis and septic arthritis rarely present concomitantly in the same joint and patient. Reactive arthritis presenting after coronavirus disease 2019 is also exceedingly rare, with less than 30 cases reported thus far. Less common pathogens such as Clostridium difficile have been reported to cause reactive arthritis, especially in patients with a positive human leukocyte antigen B27, and therefore should be considered in diagnostic algorithms. The aim of this case report is to highlight the difficulties and precautions in discerning and diagnosing patients presenting with sudden swelling of the knee. We report the case of a 70-year-old Caucasian male with a recent history of coronavirus disease 2019 upper respiratory infection and diarrhea and negating trauma, who presented with a swollen and painful knee. Pain and swelling worsened and inflammatory parameters increased…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
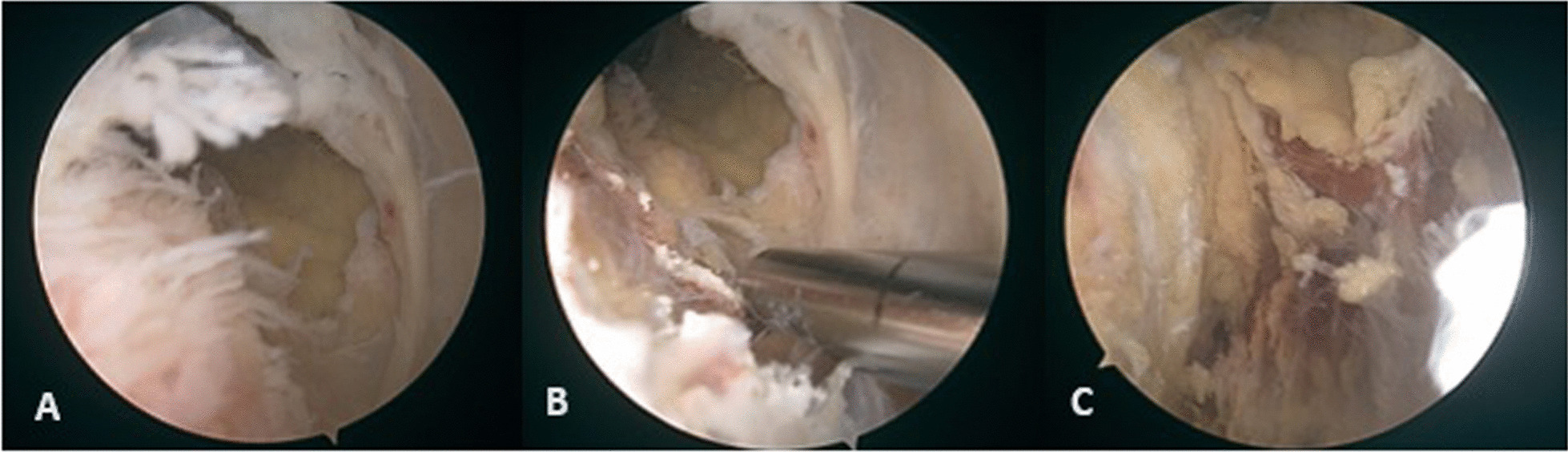 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Infections and Treatments · Clostridium difficile and Clostridium perfringens research · Infectious Diseases and Tuberculosis
Background
Septic arthritis of the knee is a condition characterized by the presence of bacteria inside the knee joint that is accompanied by a severe inflammatory reaction. Epidemiological data have shown that the incidence of septic arthritis spans 2–10 per 100,000 patients [1]. Such a condition can be hazardous for the patient, with a loss of cartilage seen as early as 8 h after infection [2]. However, the correct diagnosis of septic arthritis can be a challenging task, as other conditions may present with similar clinical findings. The following is a case report of a 70-year-old Caucasian male who presented with recurrent knee pain symptoms after an undiagnosed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection that necessitated arthroscopic lavage for high clinical and biological suspicion of septic arthritis.
Case presentation
A 70-year-old Caucasian male patient with a history of partial meniscectomy of the left knee presented to the hospital on two occasions over a period of 10 days with complaints of swelling and pain in the knee while negating any trauma or other provoking factors. During the first visit, after a synovial fluid puncture, the patient received an intraarticular corticosteroid injection, which provided relief of symptoms for a few days. More intense knee swelling was present on the second visit 7 days after the first visit. Synovial fluid was collected from the knee and was sent for analysis. A follow-up appointment was performed 3 days after the second visit, and synovial fluid analysis results revealed increased leukocytes at 10,980 × 10^6^/L. Still, the microbiological analysis was negative for the presence of bacteria. Blood results showed increased leukocytes at 20 × 10^9^/L, C-reactive protein (CRP) at 222.7 mg/L, and procalcitonin at 0.33 μg/L. The patient was admitted to the hospital on the same day for suspicion of septic arthritis. Laboratory workup confirmed a previous coronavirus disease 2019 (COVID-19) infection via analysis of cellular immunity levels, which was not recognized a month prior to hospitalization and was treated with empiric antibiotics (amoxicillin and clavulanic acid) by an ear nose throat (ENT) specialist in a different institution prior to hospitalization. The patient underwent urgent arthroscopic lavage the day after admission, revealing a cloudy synovial fluid, moderate synovitis, petechial bleeding, some fibrin accumulations, and degenerative lesions of the medial meniscus and articular cartilage (Fig. 1). The synovial fluid sample taken on the day of admission and tissue samples taken during the arthroscopy were sent for bacterial culture analysis and were found to be sterile. Furthermore, panbacterial multiplex 16 s-polymerase chain reaction (PCR) was performed on the synovial fluid and tissue samples taken intraoperatively and showed negative results for the presence of bacterial DNA as the causative agent of septic arthritis (Table 1). On the first postoperative day, Clostridium difficile toxin was isolated from the stool and oral vancomycin was introduced in part with the empiric therapy for suspected septic arthritis. Follow-up laboratory parameters were carried out several times and showed regressive dynamics of inflammatory indicators over the next 2 days. The patient was discharged on the fourth day after admission, afebrile and not complaining of knee pain. Intravenous vancomycin (1 g twice a day) and ceftriaxone (2 g once a day) for potential septic arthritis with concomitant oral vancomycin (125 mg four times a day) for C. difficile were continued for 2 weeks postoperatively, followed by a switch to 1 week of oral cephalexin (500 mg three times a day). Furthermore, several laboratory parameters, such as serum levels of rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibody levels, were evaluated, and human leukocyte antigen (HLA) testing was performed. Both anti-CCP antibodies (1.5 U/mL) and RF (< 20.0 kU/L) were below the reference interval values and therefore considered negative. The results of genetic testing for HLA revealed the presence of the HLA-B27 allele. At the follow-up visit 2 months after discharge, C. difficile toxin in the stool was tested and the result came back negative. The patient reported significant improvement in symptoms, negated any further episodes of diarrhea, and clinically showed signs of recovery.Fig. 1. Arthroscopy images taken during emergent arthroscopic lavage of the patient’s knee. a Arthroscopy image shows slight synovitis at the injection site with petechial bleeding. b Arthroscopy image after debridement of the synovitis. c Arthroscopy image revealing bleeding and necrosis at the injection siteTable 1Panel of the pathogens tested using multiplex 16 s rDNA PCRGram-negative bacteria Acinetobacter calcoaceticus—baumannii complex, Bacteroides fragilis, Enterobacterales, Enterobacter cloacae complex, Escherichia coli, Klebsiella aerogenes, Klebsiella oxytoca, Klebsiella pneumoniae group, Proteus spp., Salmonella, Serratia marcescens, Haemophilus influenzae, Neisseria meningitidis, Pseudomonas aeruginosa, Stenotrophomonas maltophiliaGram-positive bacteria Enterococcus faecalis, Enterococcus faecium, Listeria monocytogenes, Staphylococcus spp., Staphylococcus aureus, Staphylococcus epidermidis, Staphylococcus lugdunensis, Streptococcus spp., Streptococcus agalactiae, Streptococcus pneumoniae, Streptococcus pyogenesFungi Candida albicans, Candida auris, Candida glabrata, Candida krusei, Candida parapsilosis, Candida tropicalis, Cryptococcus neoformans/gattiiAdditional pathogens Campylobacter (jejuni, coli, and upsaliensis), Clostridium difficile (toxin A/B), Yersinia enterocolitica, Vibrio cholerae, V. parahaemolyticus, V. vulnificus, Shigella
Discussion and conclusion
Septic or infectious arthritis (SA) is an acute joint inflammation caused by microorganisms introduced into the joint either hematogenously or by direct inoculation. It is mainly a clinical diagnosis, and in the adult population, the main culpable microorganism is Staphylococcus aureus [3]. It is important to note that there is no consensus on how to base the diagnosis of SA in adults on laboratory values such as peripheral blood leukocytes, synovial fluid (SF), white blood cell (WBC) count, or even gram staining of the SF. All of the tests mentioned above are of moderate relevance when it comes to diagnosing the presence of a joint infection correctly [4, 5]. The role of PCR in the diagnostic algorithm is also conflictual and has to be backed by further studies [4, 6, 7].
This can make the diagnosis challenging even for highly skilled and experienced physicians. The distinction between septic and inflammatory noninfectious arthritis cannot be made on the basis of the mere observation of synovial fluid (SF). Even though literature reports that a SF WBC count of > 50.000/mm^3^ is highly indicative of infectious arthritis, this is also not a specific enough parameter for the diagnosis since numerous cases of SA have been reported with an inferior SF WBC count and gram staining that was negative for the presence of bacteria [8, 9]. The case fatality in patients with monoarticular disease, even in expert hands, is around 11%. Therefore, any patient with suspected SA should be admitted to the hospital for prompt assessment, diagnostics, and intravenous antibiotic treatment [3, 10].
Reactive arthritis (ReA), on the other contrary, is an acute non-purulent arthritis that classically presents as either sacroiliitis, enthesitis, asymmetrical oligoarthritis primarily of the lower limbs, or a combination of the above-mentioned features. It also has typical extraarticular manifestations such as urethritis, conjunctivitis, and mucocutaneous lesions of the genitalia (balanitis, keratoderma blenorrhagicum). ReA belongs to the spectrum of spondyloarthritides (SpA), which also includes ankylosing spondylitis (AS), psoriatic arthritis (PsA), and inflammatory bowel disease related arthritis (IBDa). ReA should be considered in the differential diagnosis of acute knee pain with effusion. It most commonly affects individuals 18–40 years of age. It is known to generally occur after genitourinary or gastrointestinal infections caused by microorganisms such as Chlamydia trachomatis, Salmonella enteritidis, Shigella shigae, Yersinia enterocolitica, and Campylobacter jejuni [11]. Individuals with the HLA-B27 allele or family history of ankylosing spondylitis have an increased risk of developing ReA [11]. Approximately 30–80% of ReA cases in population studies are reported in patients with a positive HLA-B27 antigen, which is also linked to other forms of the SpA spectrum such as AS and IBDa [12]. HLA-B27 is also linked with increased intestinal permeability, which may be a pathogenic mechanism for the above-mentioned pathogens [13, 14]. Clostridium difficile is a pathogen that is very rarely associated with ReA, and some viral pathogens such as parvovirus B19, chikungunya virus, hepatitis B, human immunodeficiency virus (HIV), and more recently, SARS-CoV-2 have been linked to post-viral ReA [13, 15–17]. Other viruses, including hepatitis C, rubella, mumps, Epstein–Barr virus (EBV), cytomegalovirus (CMV), herpes simplex virus (HSV) 1 and 2, and flavivirus, have been linked with arthritis as well, although the presentation of the disease mediated by these pathogens is generally acute and polyarticular [18]. It is believed that circulating antigens from the above-mentioned pathogens enter the synovium and subsequently cause the activation of synovial fluid mononuclear cells (SFMC) such as macrophages and CD4+ T-helper cells [19]. Circulating lipopolysaccharides from the bacterial membrane, microorganism DNA, and molecular mimicry of these bacterial antigens with the HLA-B27 epitope are believed to be a causing mechanism for ReA [20, 21]. Several authors describe other mechanisms for the pathogenesis of ReA for different bacterial microorganisms. Chlamydia trachomatis persists in an aberrant metabolically active form in peripheral monocytes that reach the synovium through the bloodstream from the primary site of infection [22]. In post-enteric ReA caused by invasive bacteria, there is no persistence of entire microorganisms, but rather, there is a presence of some of their structural components: outer membrane proteins (OMPs) such as porins, lipoproteins, or lipopolysaccharides of the outer membrane in the synovium and SF [23]. Both the aberrant form of C. trachomatis and the outer membrane antigens of enteric bacteria are subsequently presented to naive T-lymphocytes. This is thought to be the reason for increased SF and serum levels of cytokines such as IFN-γ, IL-1β, IL-4, IL-17, and TNF-α and the ensuing inflammation [12, 22]. The pathogenic mechanism for C. difficile ReA is still quite unclear, since the bacteria is enterotoxic (toxin A, toxin B) but not invasive. Toxin A contributes to the increased permeability of the intestinal wall through inactivation of host GTPases and therefore altering the mucosa. This finally allows for bacterial antigens to reach the bloodstream [13, 24]. This is a potential explanation as to how synovial fluid and knee swelling could occur post-C. difficile infection.
Since the breakout of COVID-19, less than 30 cases that fill the diagnostic criteria for post-viral ReA caused by SARS-CoV-2 have been reported, and the exact mechanism of this condition is still a topic for discussion [17, 25, 26]. Cellular immunity to COVID-19 is marked by a strong CD4+ TH1 cell response, secreting high levels of IFN-γ [27]. Some studies have proven that the synovial inflammation in ReA is primarily mediated by synovial CD4+ TH2 cells secreting interleukin-10, which consequently decreases the TH1 secretion of IFN-γ in the acute phase [12, 22, 28]. This correlates with a longer persistence of microorganisms in the SF [28–30]. No studies have yet been conducted on the effects of SARS-CoV-2 antigens on SFMC. It is possible that SARS-CoV-2 shares a myeloid cell activation pathway with other rheumatological diseases, which may contribute to some of its arthritic presentations, though rare, and to the elevated neutrophil count in the SF [31].
The patient developed arthritic symptoms 3.5 weeks after a COVID-19 upper respiratory tract infection that was treated with amoxicillin and clavulanic acid. The patient also reported post-antimicrobial diarrhea lasting for a week, which was highly probably caused by C. difficile. Increased CRP levels (222.7 mg/L), backed by an elevated procalcitonin, are regarded as highly indicative of an active bacterial infection and alerts to the possibility of a septic joint infection in cases of a painful and debilitating joint effusion. Relapsing joint effusions, over a period of 10 days after the intraarticular corticosteroid injections, indicate the possibility that the arthritis was not caused exclusively due to a reactive, rheumatologic condition. Treatment with intravenous antibiotics (vancomycin and ceftriaxone) for the plausible SA, and oral vancomycin for the eradication of C. difficile, were initiated immediately to cover both of the potential causes of arthritis. The antibiotic therapy was well tolerated by the patient; adverse effects included only slight nausea. Such intervention was necessary for the prevention of possible devastating effects of SA on the knee joint while allowing for an adequate diagnostic evaluation of other conditions included in the differential. As the HLA testing revealed the presence of HLA-B27 antigen, commonly associated with ReA, and since the results of both panbacterial PCR and bacterial culture of the synovial fluid and the synovium came back negative, ReA emerged as an even more plausible cause of the symptoms. However, the quick regression of knee pain and swelling, as well as the immediate drop in CRP levels after antibiotic therapy, does not allow us to exclude SA as a potential cause.
The distinction between diagnoses remains unclear, and so too the pathogen possibly causing ReA; whether it is SARS-CoV-2 or C. difficile. However, significant improvement in symptoms 2 months after discharge shows that the therapy was efficacious. Nevertheless, the lack of a histopathological analysis of a tissue biopsy prevents a definitive diagnosis of reactive arthritis. However, the absence of an isolated microorganism is most probably indicative of reactive arthritis. Synovial fluid results were neither in favor of septic nor reactive arthritis. As a result, regarding and treating the patient as a patient with SA prevented any complications of a possible SA infection. This case shines a light on the necessity to consider ReA in the differential diagnosis of joint effusion. It is also indispensable to contemplate the possibility of ReA presenting after infections with less common pathogens, such as C. difficile and SARS-CoV-2.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vassallo C Borg AA Farrugia D Mercieca C The epidemiology and outcomes of septic arthritis in the Maltese islands: a hospital-based retrospective cohort study Mediterr J Rheumatol 20203119510.31138/mjr.31.2.19532676557 PMC 7362118 · doi ↗ · pubmed ↗
- 2Elsissy JG Liu JN Wilton PJ Nwachuku I Gowd AK Amin NH Bacterial septic arthritis of the adult native knee joint JBJS Rev 20208 e 0059 e 005910.2106/JBJS.RVW.19.0005931899698 · doi ↗ · pubmed ↗
- 3Mathews CJ Weston VC Jones A Field M Coakley G Bacterial septic arthritis in adults Lancet 201037584685510.1016/S 0140-6736(09)61595-620206778 · doi ↗ · pubmed ↗
- 4Carpenter CR Schuur JD Everett WW Pines JM Evidence-based diagnostics: adult septic arthritis Acad Emerg Med 20111878179610.1111/j.1553-2712.2011.01121.x 21843213 PMC 3229263 · doi ↗ · pubmed ↗
- 5Long B Koyfman A Gottlieb M Evaluation and management of septic arthritis and its mimics in the emergency department West J Emerg Med 20192033134110.5811/westjem.2018.10.4097430881554 PMC 6404712 · doi ↗ · pubmed ↗
- 6Yang S Ramachandran P Hardick A Hsieh Y-H Quianzon C Kuroki M Hardick J Kecojevic A Abeygunawardena A Zenilman J Rapid PCR-based diagnosis of septic arthritis by early gram-type classification and pathogen identification J Clin Microbiol 2008461386139010.1128/JCM.02305-0718305128 PMC 2292921 · doi ↗ · pubmed ↗
- 7Jacquier H Fihman V Amarsy R Vicaut E Bousson V Cambau E Crémieux A-C Delcey V Hannouche D Kaci R Benefits of polymerase chain reaction combined with culture for the diagnosis of bone and joint infections: a prospective test performance study Open Forum Infect Dis 201910.1093/ofid/ofz 51131909081 PMC 6935679 · doi ↗ · pubmed ↗
- 8Mc Gillicuddy DC Shah KH Friedberg RP Nathanson LA Edlow JA How sensitive is the synovial fluid white blood cell count in diagnosing septic arthritis?Am J Emerg Med 20072574975210.1016/j.ajem.2006.12.00117870475 · doi ↗ · pubmed ↗