Early Mobilization and Rehabilitation to Enhance the Functional Performance of a Hemiparesis Patient Following a Subdural and Subarachnoid Hematoma With Pneumocephalus: A Case Report
Disha K Rathi, Shraddha S Kochar, Snehal Samal, Akshaya Saklecha

TL;DR
This case report shows how physiotherapy helped a patient recover from a brain injury causing hemiplegia.
Contribution
The study highlights the effectiveness of early physiotherapy in improving recovery for a complex brain injury case.
Findings
The patient's lower limb strength improved significantly after physiotherapy.
Physiotherapy is critical for enhancing muscle strength and recovery in such cases.
Abstract
A subdural hematoma (SDH) is a medical condition caused by a violent head trauma in which blood accumulates excessively under the dura mater. It occurs when a blood arterial weak point or brain surface aneurysm ruptures and bleeds. The resulting blood accumulation inside and around the skull raises the pressure on the brain. Pneumocephalus, also known as pneumatocele or intracranial aerogel, refers to air in the ventricular cavities or brain parenchyma's epidural, subdural, or subarachnoid spaces. In most cases, neurotrauma is the primary cause of pneumocephalus, mainly when there are skull base fractures. Here, we present a case study of a 65-year-old male patient diagnosed with left hemiplegia following SDH with subarachnoid hematoma (SAH) and pneumocephalus. The severity of the patient's illness, the medical and surgical care provided, the amount of physiotherapy required to aid…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
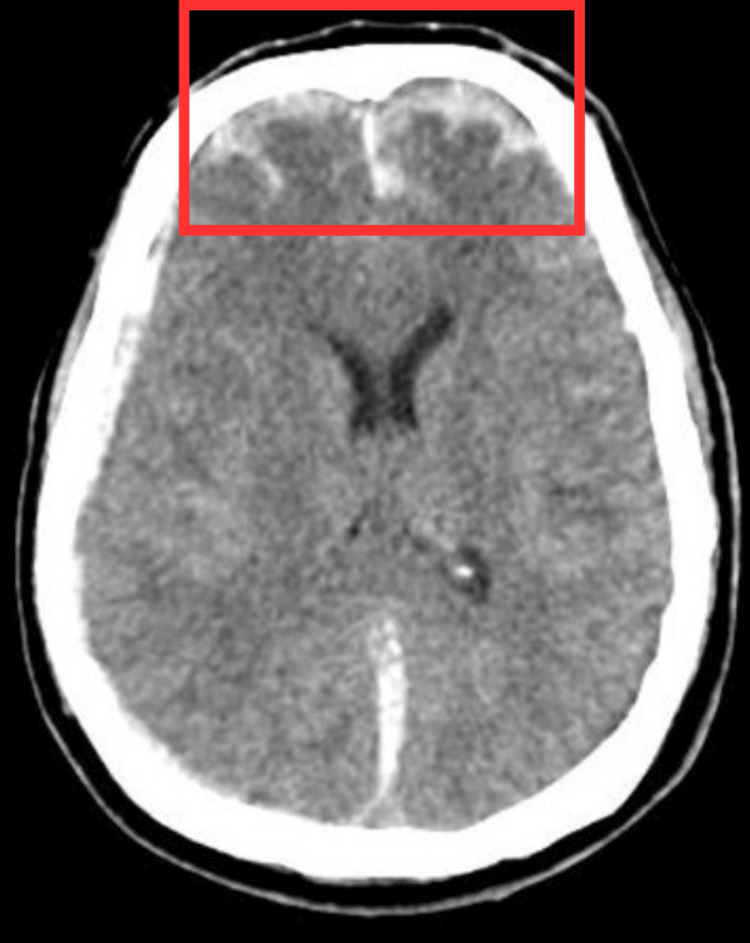 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3| Pre-rehabilitation | Post-rehabilitation | ||||
| Side | Lower limb | Upper limb | Side | Lower limb | Upper limb |
| Right | 2+ | 2+ | Right | 2+ | 2+ |
| Left | 1+ | 1+ | Left | 2+ | 2+ |
| DTR | Pre-rehabilitation | Post-rehabilitation | ||
| Reflexs | Right | Left | Right | Left |
| Biceps jerk | + | + | ++ | ++ |
| Triceps jerk | + | + | ++ | ++ |
| Knee jerk | + | + | ++ | ++ |
| Ankle jerk | + | + | ++ | ++ |
| Plantar jerk | Flexor response | Extensor response | Flexor response | Flexor response |
| VCG | Pre-rehabilitation | Post-rehabilitation | ||
| Limb | Right | Left | Left | Left |
| Upper limb | Grade 2 | Grade 1 | Grade 5 | Grade 4 |
| Lower limb | Grade 2 | Grade 1 | Grade 5 | Grade 4 |
| Goals | Therapeutic interventions | Treatment protocol | Dosage |
| To normalize the tone of muscles | Rood’s approach was given | Joint approximation to left upper and lower limb joints | 10 reps |
| PNF to left upper and lower limb | Rhythmic initiation technique was given to correct the muscle imbalance and restore the patient’s ability to perform effective coordinated movement. A D1 flexion-extension pattern was used. | 10 reps with 2 sets | |
| Progression was given with PNF in combinations of isotonic to slow reversal. | 10 reps with 2 sets | ||
| To enhance mobility | ROM | PROM exercises were commenced. | 10 reps twice a day |
| To prevent DVT | Ankle exercises | Passive ankle pumps along with heel slides and DVT stockings | 20 reps three times a day |
| Bronchial hygiene | Chest physiotherapy | Positioning, manual chest techniques (percussion and vibrations), and suctioning was given. | Change in position every 2-3 hours and manual techniques for 10 reps thrice a day |
| Prevention of contracture | Prolonged splinting and positioning | Sustained stretch to tendo-achilles | Relaxation for 10 seconds and hold time for 30-40 seconds |
| To prevent bed sores and to improve bed mobility | Segmental rolling techniques | Rolling facilitation that included rolling from supine to side-lying using upper extremity momentum and crossing the ankle pattern. Transition training from supine to sitting that inluded prone on the elbows from prone on elbows to long sitting, use elbow walking, supine on elbows. | Change in position in every 2-3 hours |
| Outcome measures | Pre-rehabilitation | Post-rehabilitation |
| GCS | 8/15 | 12/15 |
| FIM | 35/126 | 102/126 |
| CRS | 8/23 | 18/23 |
| MMSE | 18/30 | 26/30 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurosurgical Procedures and Complications · Intracerebral and Subarachnoid Hemorrhage Research · Head and Neck Surgical Oncology
Introduction
A subdural hematoma (SDH) is the accumulation of blood between the dura and the arachnoid membranes [1]. It is categorized into three groups, namely, chronic, sub-acute, and acute, with injury to the head being the primary cause of acute SDH [2]. Several factors, including injury, arteriovenous malformation, and anticoagulant substance use, can lead to SDH [3]. The categorization of SDH is based on the size, location, and time elapsed since the initiating event [4]. SDH has a high fatality rate and significant long-term morbidity, with up to 32 percent (%) death rate and a 33% recurrence rate [5]. The underlying cause of SDH is believed to be the cortical veins that bridge the subdural space and empty into the nearby dural sinus, which stretch and tear when the head's velocity suddenly changes, leading to shearing forces and vein rupture. The arachnoid can also tear, resulting in a mixture of cerebrospinal fluid (CSF) and blood in the subdural space [6]. The collection of blood between the arachnoid and pia mater can cause potentially fatal subarachnoid hemorrhages (SAH), with aneurysm rupture being the leading cause of SAH in 85% of cases [7].
The clinical presentation of SDH varies, with the most common symptom being a sudden, severe headache accompanied by meningism, temporary or prolonged unconsciousness, and specific neurological impairments, such as paresis and cranial nerve palsies [8]. Hemorrhagic strokes constitute 20% of all strokes, with 10% being SAH and 10% being intracerebral hemorrhage (ICH). Acute death due to SAH is caused by blood accumulation between the arachnoid and the pia mater. Ten to 14 out of every 100,000 people experience SAH in the United States each year [9]. SAH is more common in women, with a ratio of 3:1, but men are more likely to have it before the age of 40. Aneurysmal rupture is more common as individuals age, peaking in the fifth and sixth decades. The risk of bleeding in individuals with a previously unruptured aneurysm is 1% to 2% per year, with a higher risk for aneurysms more giant than 7 millimeters [10]. Hypertension and cocaine use are linked to ICH and aneurysmal rupture. The presence of air in the ventricular cavities is known as pneumocephalus, which can occur spontaneously, after brain surgery, or as a result of trauma [11]. It can be classified as simple or tension pneumocephalus, and in clinical settings, it can cause headaches, nausea, vomiting, agitation, lightheadedness, and convulsions [12]. Based on the sound of gas input, patients sometimes describe air entry into the cerebral space as a "gurgling" sensation in the head [13].
Our data collection included 1,307 SDH patients, 805 of whom had a history of head trauma, while 502 did not. Physiotherapy plays a critical role in rehabilitation, and an algorithm for step-by-step mobilization was used to enable early mobilization starting from the day following aneurysm repair [14]. Early rehabilitation of patients following SAH is safe and feasible, and higher degrees of mobilization do not increase neurosurgical complications. Instead, early rehabilitation reduces the frequency and severity of cerebral vasospasm following an SAH [15]. The field of neurorehabilitation for traumatic brain injury (TBI) is extensive and complicated, encompassing early patient rehabilitation for those with compromised cognitive, motor, sensory, and communicative function due to nervous system issues, as well as patient support and reintegration into their social and professional contexts [16].
Case presentation
Patient information
A 65-year-old male, an auto-rickshaw driver, was seen following a road traffic accident (RTA) with a pedestrian early in the morning. The patient was found unconscious at the site of the incident and taken to hospital. He had a history of trauma, nasal bleeding, and a right ear bleed. There was no history of fever, vomiting, or seizures. After examination, the patient’s Glasgow Coma Scale (GCS) score was 3/15 (E1V1M1). The patient was seen within minutes for a neurology assessment, and a computed tomography (CT) scan of the skull revealed SDH and SAH, and the patient was managed conservatively. Antibiotics, antiemetics, analgesics, antifibrinolytics, and antacids are among the medications administered during the patient’s conservative care, and the patient was on 6 liters of oxygen via a facemask.
Clinical findings
Before the commencement of the physical examination, the patient provided his informed consent and subsequently underwent the assessment. Throughout the examination, the patient displayed a cooperative demeanor and demonstrated a clear orientation to place, person, and time, with a GCS score of 8 out of 15. The patient was positioned in a supine state and remained hemodynamically stable throughout the assessment. During the neurological examination, a reduction in tone was observed in the left upper and lower limbs (as depicted in Table 1). All deep tendon reflexes were noted to be diminished (as shown in Table 2). The voluntary grading scale (VCG) revealed a half range of motion (ROM) in synergy on the right side, while the left side displayed the initiation of movement (as detailed in Table 3). In addition, Babinski’s sign was noted to be positive. Based on these findings, a clinical diagnosis of hemiparesis on the left side was made, rendering the patient unable to stand or walk. Furthermore, the functional independence measure (FIM) indicated that the patient required maximal assistance with basic activities of daily living (ADLs). Consequently, the patient was referred for neurophysiotherapy.
Diagnostic assessment
A CT scan revealed a fracture in the occipital bone accompanied by swelling. In addition, fractures were observed in the right temporal bone along the petrous bone and mastoid process. Furthermore, hyperdense SDH was detected along the interhemispheric fissure and tentorial lining. A hyperdense hemorrhagic contusion was also observed in the bilateral temporal and frontal regions. Focal SAH was identified along the bilateral frontoparietal and Parisian fissure. Mild mucosal thickening was noted on both sides of the ethmoid and maxillary sinuses (Figure 1).
Computed tomography scan of the brain.The red rectangle shows a subdural hematoma on the left side.
Physiotherapy intervention
A tailored rehabilitation protocol was developed for the patient to address their needs. The patient underwent physiotherapy for four weeks, with sessions occurring five days a week. Table 4 outlines the details of the physical therapy protocol that was implemented. In Figure 2, the therapist can be seen administering upper limb proprioceptive neuromuscular facilitation (PNF) therapy to the patient. In addition, Figure 3 depicts the therapist assisting the patient with bed mobility exercises.
Proprioceptive neuromuscular facilitation
Bed mobility exercise
Follow-up and outcome measures
During the fourth week of rehabilitation, the patient was subjected to a follow-up assessment, wherein outcome measures were estimated before and after the rehabilitation process. Table 5 shows the detailed information on these measures.
Discussion
The incidence of SAH commonly occurs at the rate of 10-20 per 100,000 individuals, with the average age of patients being 50 years old [17]. Based on the study, early mobilization was established as feasible after proper safety screening, and almost all the participants could achieve higher mobility or sit at the edge of their bed at least once during their physiotherapy period. In addition, half of the physiotherapy interventions allowed for mobilization. However, neurological factors, such as moderate sleepiness or recent or impending neurological surgery, often hinder mobilization. It was found that most of the participants who could be mobilized advanced to walking four to five days after admission, and all of them had crossed the mobility milestone of sitting on the side of the bed. Unfavorable incidents linked to mobilization were few, fleeting, and self-limiting [18].
Saciri et al. (2002) conducted a study revealing significant variations in the severity of sickness, medical and surgical care, quantity of physiotherapy, length of hospital stay, and place of release among patients with acute SAH or SDH [19]. According to Karic et al. (2015), patients with non-traumatic SAH can benefit from an early mobility program emphasizing upright sitting, standing, walking, functional training, and therapeutic supine activities [20]. Therefore, early mobilization can be considered safe and practical for such patients.
This care report pertains to a patient with concurrent subdural and subarachnoid hematoma. Neurorehabilitation is a multifaceted field encompassing patient support, reintegration into social and professional contexts, and early rehabilitation of patients with compromised motor, cognitive, sensory, and communicative functions caused by nervous system disorders. The patient was subjected to a rhythmic initiation technique to correct muscle imbalances and restore the patient’s ability to perform effective coordinated movement. The primary goal of physical therapy was to enhance muscle mobility. To prevent contractures, prolonged splinting and positioning were administered. Upon admission to the hospital, the patient scored 18 on the Mini-Mental Scale Examination but increased to 26 following therapy sessions. The patient experienced cognitive impairment, but as his cognition improved, his conscious level also increased.
Conclusions
This report provides evidence that patients with cerebral hemorrhage exhibit better prognoses when they engage in prompt mobilization and adhere to recommended physical therapy regimens. In addition, their quality of life (QOL) improves. The physiotherapeutic interventions employed in this case were highly effective, with a reasonable recovery rate that improved the patient’s QOL, muscle strength, and mobility. Patients can achieve a higher QOL when they receive physiotherapy tailored to their individual needs and objectives, focusing on enhancing function, engagement, and symptom management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prognostic factors after acute subdural hematoma J Trauma Dent DL Croce MA Menke PG 363391995763690810.1097/00005373-199507000-00005 · doi ↗ · pubmed ↗
- 2Nontraumatic bilateral subdural hematoma: case report Ann Med Surg (Lond) Mohamed T Swed S Al-Mouakeh A Sawaf B 71202110.1016/j.amsu.2021.102907 PMC 852867434712475 · doi ↗ · pubmed ↗
- 3Chronic subdural hematoma Asian J Neurosurg 10 2024 Yadav YR Parihar V Namdev H Bajaj J 3303421120162769553310.4103/1793-5482.145102 PMC 4974954 · doi ↗ · pubmed ↗
- 4The surgical management of chronic subdural hematoma Neurosurg Rev 10 2024 Ducruet A Grobelny B Zacharia B 1151201110.1007/s 10143-011-0349-y 21909694 · doi ↗ · pubmed ↗
- 5Chronic subdural hematoma: epidemiology and natural history Neurosurg Clin N Am 11 2024 Yang W Huang J 2052102820172832545410.1016/j.nec.2016.11.002 · doi ↗ · pubmed ↗
- 6Subarachnoid hemorrhage and intracerebral hematoma: incidence, prognostic factors, and outcome Neurosurgery Güresir E Beck J Vatter H Setzer M Gerlach R Seifert V Raabe A 108810936320081905732010.1227/01.NEU.0000335170.76722.B 9 · doi ↗ · pubmed ↗
- 7Subarachnoid hemorrhage Stat Pearls [Internet] Ziu E Suheb M Mesfin F Treasure Island (FL)Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 441958/28722987 · pubmed ↗
- 8Subarachnoid hemorrhage: clinical presentation and neuropsychological outcome Med Update Psychiatr Bernardini G Mayer S 717631998