The Impact COVID-19 Infection on Cancer Patients: A Tertiary Cancer Center Experience in Jordan
Kamal Al-rabi, Fadwa Al-Qadi, Akram Al-Ibraheem, Khalid Halahleh, Samer Salah, Hazim Ababneh, Mohammad Akkawi, Maher Sughayer, Lana Tafesh, Layan Abu Abed, Mohammad Ma'koseh

TL;DR
This study examines how COVID-19 affects cancer patients in Jordan, finding high mortality and treatment disruptions.
Contribution
The study provides insights into the impact of COVID-19 on cancer patients in a low- to middle-income country context.
Findings
31.8% of cancer patients with COVID-19 required hospitalization, and 15.8% died.
Low albumin and leucocytosis were strongly associated with higher mortality.
Recent chemotherapy was linked to better survival in patients with active cancer.
Abstract
Background: Cancer patients are at higher risk of serious complications of COVID-19. Few studies evaluated the impact of COVID-19 on cancer patients in low- and middle-income countries. Our study aims to evaluate the outcomes of COVID-19 infection in cancer patients treated at our institution. Methods: Medical records of patients with a positive COVID-19 polymerase chain reaction (PCR) between April 2020 and October 2020 were reviewed. Fisher's exact test and logistic regression analysis were employed to correlate various variables with mortality. Survival estimates were generated using the Kaplan-Meier method. Results: A total of 317 patients were included, with a median age was 55 years (range: 19-88). 82 (25.9%) had hematological neoplasms while the remainder had solid cancers. At the time of infection, 220 (69.4%) had active cancer, and 99 (31.2%) had received systemic anticancer…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
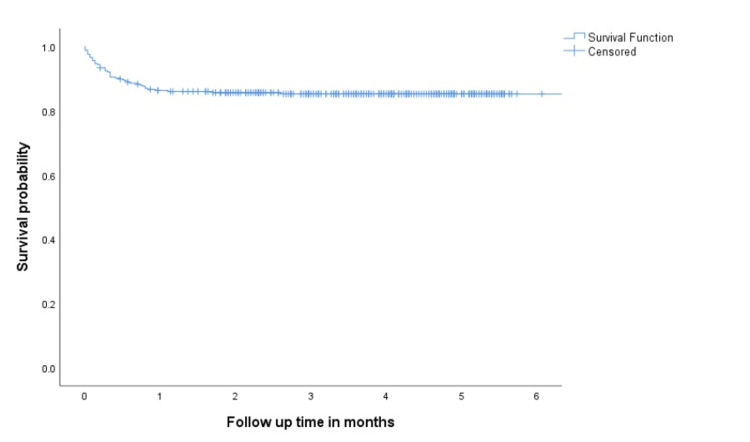 Figure 1
Figure 1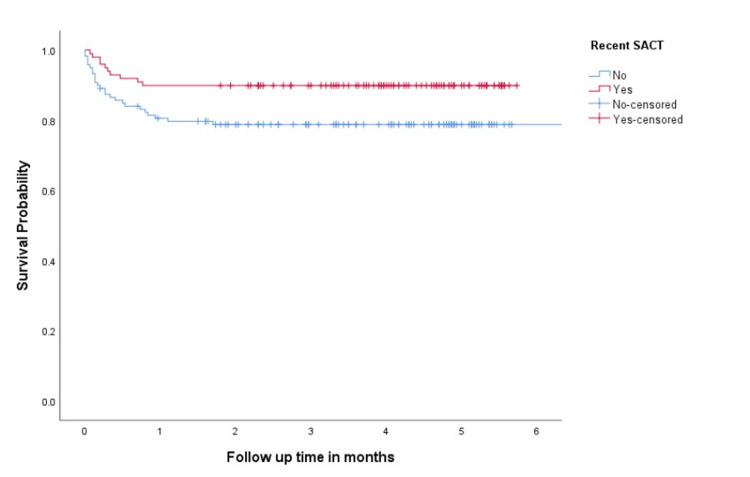 Figure 2
Figure 2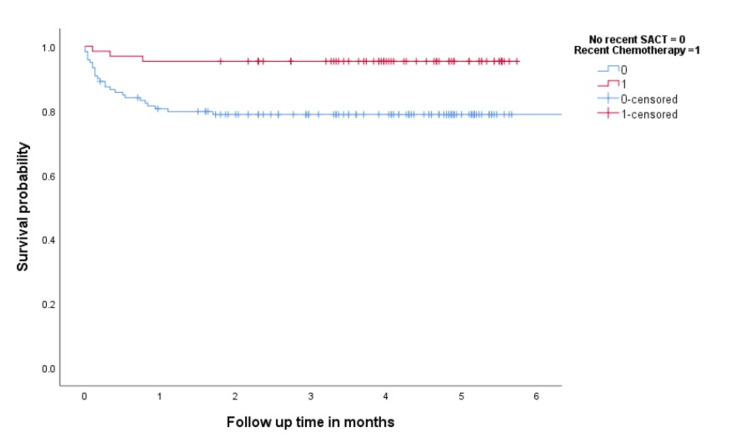 Figure 3
Figure 3| Characteristic | Number (%) |
| Male | 142 (44.8%) |
| Female | 175 (55.2%) |
| Age > 60 | 116 (36.6%) |
| BMI > 30 | 139 (43.9%) |
| Current or ex-smoker | 130(41%) |
| Comorbidities | 197 (62.1%) |
| Diabetes mellitus | 90 (28.4%) |
| Hypertension | 121 (38.2%) |
| Cardiovascular disease | 39 (12.3%) |
| Chronic obstructive lung disease | 10 (3.2%) |
| Chronic kidney disease | 21 (6.6%) |
| Other comorbidities* | 27 (8.5%) |
| Solid cancer | 235 (74.1%) |
| Hematological neoplasm | 82 (25.9%) |
| Active cancer | 220 (69.4%) |
| Lung cancer | 16 (5%) |
| Breast cancer | 88 (27.8%) |
| Gastrointestinal cancers | 47 (14.8%) |
| Genitourinary cancer | 35 (11%) |
| Head and neck cancer | 16 (5%) |
| Gynaecological cancer | 14 (4.4%) |
| Sarcoma | 6 (1.9%) |
| Non-Hodgkin lymphoma | 26 (8.2%) |
| Hodgkin lymphoma | 9 (2.8%) |
| Leukaemia | 26 (8.2%) |
| Multiple myeloma | 19 (6%) |
| Other cancers | 15 (4.7%) |
| No SACT within 4 weeks | 218 (68.8%) |
| Haemoglobin < 10 grams/dl | 86 (27.2%) |
| WBC count > 11/µl | 107 (33.7%) |
| WBC count < 4/µl | 110 (34.7%) |
| Neutrophil count < 1,000/µl | 49 (15.4%) |
| Lymphocyte count < 1,000/µl | 198 (62.4%) |
| Lymphocyte count < 500/µl | 85 (26.8%) |
| High ALT | 27 (8.5%) |
| High AST | 38 (12%) |
| High bilirubin | 21 (6.6%) |
| Albumin ≤ 3.5 grams/dl | 130 (41%) |
| Variable | Alive % | Dead % | P value |
| Male | 40% | 58.1% | 0.018 |
| Female | 60% | 41.9% | |
| Age ≤ 60 | 67.4% | 42% | 0.001 |
| Age > 60 | 32.6% | 58% | |
| BMI ≤ 30 | 56.9% | 53.1% | 0.617 |
| BMI > 30 | 43.1% | 46.9% | |
| Current or ex-smoker | 60% | 51.2% | 0.297 |
| Never smoked | 40% | 48.2% | |
| Diabetes mellitus | 25.5% | 44% | 0.008 |
| No diabetes mellitus | 74.5% | 56.% | |
| Hypertension | 34.5% | 66% | 0.005 |
| No hypertension | 65.5% | 44% | |
| Cardiovascular disease | 10.9% | 20% | 0.071 |
| No cardiovascular disease | 89.1% | 80% | |
| Chronic lung disease | 3% | 4% | 0.709 |
| No chronic lung disease | 97% | 96% | |
| Chronic kidney disease | 4.1% | 29% | <0.001 |
| No chronic kidney disease | 95.9% | 80% | |
| Other comorbidities | 9.7% | 2% | 0.095 |
| No other comorbidities | 90.3% | 98% | |
| Solid tumour | 77.2% | 58% | 0.005 |
| Hematological tumour | 22.8% | 42% | |
| Lung cancer | 4.9% | 6% | 0.737 |
| Other cancer | 95.1% | 94% | |
| Active cancer | 68.2% | 76% | 0.27 |
| Remission | 31.2% | 24% | |
| Haemoglobin ≥ 10 g/dl | 78.1% | 59.6% | 0.017 |
| Haemoglobin < 10 g/dl | 21.9% | 40.4% | |
| WBC count > 11/µl | 5.3% | 38.3% | <0.001 |
| WBC count ≤ 11/µl | 94.7% | 61.7% | |
| WBC count ≥ 4/µl | 59.6% | 78.7% | 0.021 |
| WBC count < 4 /µl | 40.4% | 21.3% | |
| Neutrophil count ≥ 1,000/µl | 82.5% | 89.1% | 0.293 |
| Neutrophil count < 1,000/µl | 17.5% | 10.9% | |
| Lymphocyte count ≥ 1,000/µl | 39.5% | 32.6% | 0.417 |
| Lymphocyte count <1000/µl | 60.5% | 67.4% | |
| Lymphocyte count ≥ 500/µl | 78.9% | 56.5% | 0.004 |
| Lymphocyte count < 500/µl | 21.1% | 43.5% | |
| Normal ALT | 94.1% | 85.1% | 0.073 |
| High ALT | 5.9% | 14.9% | |
| Normal AST | 91.1% | 78.7% | 0.036 |
| High AST | 8.9% | 23.3% | |
| Normal bilirubin | 96% | 87.2% | 0.075 |
| High bilirubin | 4% | 12.8% | |
| Albumin ≤ 3.5 g/dl | 75.2% | 21.3% | <0.001 |
| Albumin >3.5 g/dl | 24.8% | 78.7% | |
| Impact on SACT | 41.5% | 77.6% | <0.001 |
| No impact on SACT | 58.5% | 22.4% |
| Variable | Hazard ratio | 95% confidence interval | P value | |
| Lower | Upper | |||
| Male gender | .988 | .337 | 2.899 | 0.982 |
| Age > 60 years | 1.374 | .452 | 4.177 | 0.575 |
| Diabetes mellitus | 2.388 | .769 | 7.412 | 0.132 |
| Hypertension | 2.505 | .772 | 8.135 | 0.126 |
| Chronic kidney disease | 1.283 | .269 | 6.132 | 0.754 |
| Hematological neoplasm | 2.336 | .585 | 9.322 | 0.064 |
| High AST | 2.336 | .585 | 9.322 | 0.23 |
| Low albumin | 14.926 | 4.745 | 46.954 | < 0.001 |
| Leucocytosis | 11.992 | 3.167 | 45.416 | < 0.001 |
| Lymphocyte count < 500/µl | 2.657 | .883 | 7.990 | 0.082 |
| Hemoglobin < 10 g/dl | .721 | .236 | 2.204 | 0.566 |
| Variable | Alive % | Dead % | P value |
| Male | 40.1% | 57.9% | 0.04 |
| Female | 59.9% | 42.1% | |
| Age ≤ 60 years | 60.2% | 47.4% | 0.01 |
| Age > 60 years | 30.8% | 52.6% | |
| BMI ≤ 30 kg/m2 | 57.5% | 57.9% | 0.97 |
| BMI > 30 kg/m2 | 42.5% | 42.1% | |
| Current or ex-smoker | 60.7% | 54.8% | 0.55 |
| Never smoked | 39.3% | 45.2% | |
| Diabetes mellitus | 22% | 36.8% | 0.053 |
| No diabetes | 78% | 63.2% | |
| Hypertension | 30.8% | 50% | 0.023 |
| No hypertension | 69.2% | 50% | |
| Cardiovascular disease | 11% | 15.8% | 0.404 |
| No cardiovascular disease | 89% | 84.2% | |
| Chronic lung disease | 2.2% | 2.6% | 0.87 |
| No chronic lung disease | 97.8% | 97.4% | |
| Chronic kidney disease | 4.4% | 15.8% | 0.019 |
| No chronic kidney disease | 95.6% | 84.2% | |
| Other comorbidities | 11% | 2.6% | 0.111 |
| No other comorbidities | 89% | 97.4% | |
| Solid cancer | 81.9% | 55.3% | <0.001 |
| Hematological neoplasm | 18.1% | 44.7% | |
| Lung cancer | 5.5% | 5.3% | 0.954 |
| Other cancers | 94.5% | 94.7% | |
| No SACT within 4 weeks | 51.1% | 73.3% | 0.025 |
| SACT within 4 weeks | 48.9% | 26.7% | |
| Haemoglobin ≥ 10 g/dl | 77.2% | 56.8% | 0.02 |
| Haemoglobin < 10 g/dl | 22.8% | 43.2% | |
| WBC count > 11/µl | 97.8% | 64.9% | <0.001 |
| WBC count ≤ 11/µl | 2.1% | 35.1% | |
| WBC count ≥ 4/µl | 43.5% | 18.9% | 0.009 |
| WBC count < 4 /µl | 56.5% | 81.1% | |
| Neutrophil count ≥ 1,000/µl | 80.4% | 88.9% | 0.254 |
| Neutrophil count < 1,000/µl | 19.6% | 11.1% | |
| Lymphocyte count ≥ 1,000/µl | 40.2% | 27.8% | 0.189 |
| Lymphocyte count < 1000/µl, | 59.8% | 67.2% | |
| Lymphocyte count ≥ 500/µl | 78.3% | 52.8% | 0.004 |
| Lymphocyte count < 500/µl | 21.7% | 47.2% | |
| Normal ALT | 92.9% | 86.5% | 0.261 |
| High ALT | 7.1% | 13.5% | |
| Normal AST | 90.5% | 78.4% | 0.07 |
| High AST | 9.5% | 21.6% | |
| Normal bilirubin | 95.2% | 86.5% | 0.091 |
| High bilirubin | 4.8% | 13.5% | |
| Albumin > 3.5 g/dl | 77% | 16.2% | <0.001 |
| Albumin ≤ 3.5 g/dl | 23% | 73.8% |
| Variable | Hazard ratio | 95% confidence interval | P value | |
| Lower | Upper | |||
| Male gender | 1.255 | .311 | 5.062 | 0.749 |
| Age > 60 years | 1.166 | .276 | 4.919 | 0.834 |
| Hypertension | 6.252 | 1.271 | 30.744 | 0.024 |
| Chronic kidney disease | 1.169 | .113 | 12.113 | 0.896 |
| Hematological neoplasm | 6.198 | 1.200 | 32.021 | 0.029 |
| Low albumin | 35.881 | 6.977 | 184.533 | < 0.001 |
| Leucocytosis | 19.745 | 2.996 | 130.114 | 0.002 |
| Lymphocyte count < 500/µl | 13.386 | 2.298 | 77.978 | 0.004 |
| Hemoglobin < 10 g/dl | 1.225 | .303 | 4.951 | 0.776 |
| Recent SACT | 7.345 | 1.431 | 37.698 | 0.017 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and healthcare impacts · Economic and Financial Impacts of Cancer · COVID-19 Clinical Research Studies
Introduction
SARS-CoV-2, first identified in December 2019, triggered a global pandemic of a respiratory illness known as COVID-19 [1]. The pandemic resulted in significant morbidity and mortality including 6.9 million deaths [2]. In addition, many aspects of healthcare delivery were disrupted, and hospitals and ICUs were overwhelmed.
Cancer patients are more susceptible to getting infected with SARA-CoV-2, and they are at higher risk for COVID-19 infection-related morbidity and mortality as they are generally older, have coexisting comorbidities and immunocompromised because of their underlying malignancy or due to systemic anticancer treatment (SACT) [3-5].
Forecasting the progression of COVID-19 in cancer patients presents a challenge due to the variable extent of additional health decline. A meta-analysis encompassing data from 20 distinct studies revealed a broad range in COVID-19 related mortality among cancer patients, varying from 5.9% to 50% [6]. Beyond age and comorbidities, various cancer-related variables were identified as associated with increased mortality. For instance, Lee et al. reported that patients with hematological malignancies infected with COVID-19 exhibited a worsened clinical condition and an increased risk of death compared to those without COVID-19 infection [7]. In another study, both hematological malignancies and lung cancer patients had increased risk of severe COVID-19 infection [8]. Additionally, Kong et al. reported that patients with lung adenocarcinoma were more susceptible to SARS-CoV-2 infection than patients with lung squamous cell carcinoma [9].
Moreover, the effect of recent SACT on the outcomes of COVID-19 infection in cancer patients remains unclear. While initial studies suggested an association between SACT administration and an increased risk of death due to COVID-19, recent studies have found no adverse effects of recent SACT [8,10-14].
Few studies reported the outcomes of cancer patients infected with SARS-CoV-2 in low- and middle-income countries. Jordan is a middle-income country with limited resources [15]. The King Hussein Cancer Center is a tertiary healthcare center that provides care for about 60% of cancer cases in Jordan [16]. Herein, we report the outcomes of cancer patients infected with SARS-CoV-19 at our center.
Materials and methods
Files and medical records of adult cancer patients (>18 years) with a positive polymerase chain reaction (PCR)-confirmed SARS-CoV-2 infection from April 2020 to October 2020 were retrospectively reviewed. The data included both in-patients and out-patients. Various demographic, cancer, and therapy-related variables, along with initial laboratory tests at the time of COVID-19 diagnosis, the need for hospitalization, and ICU admission were collected. Indications for hospitalization included hypoxia and/or hemodynamic instability. Patients with metastatic neoplasm and those receiving SACT were considered to have active cancer. Recent SACT was defined as administration of systemic chemotherapy, hormonal therapy, target therapy, or immunotherapy within four weeks of COVID-19 diagnosis. Mortality was defined as death within six months of COVID diagnosis. Delayed SACT was defined as postponing SACT for more than one week.
Patient characteristics were tabulated and presented in numbers and percentages. The correlation between different variables and mortality was done using Fisher’s exact test. The variables found to have significant association with mortality (p<0.05) by univariate analysis, were subsequently entered into the multivariate logistic regression model. Survival was calculated from the time from the diagnosis of COVID 19 infection till the last follow-up, and was estimated using the Kaplan-Meier method.
The study was approved by the King Hussein Cancer Centre Institutional Review Board (IRB) in compliance with the principles of the Declaration of Helsinki. A waiver of the written informed consent was granted due to the retrospective nature of the review, and the data were anonymized and maintained with confidentiality.
Results
Patients’ characteristics
A total of 317 patients were included with a median age of 55 (range: 19-88) years and an almost equal gender distribution. The PCR test was indicated in 191 individuals (60.3%) presenting COVID-19-related symptoms. For the remaining patients, testing was conducted electively, either before scheduled surgeries or elective procedures, or after potential exposure to COVID-19-infected individuals. A total of 235 patients (74%) had solid malignancies, whereas 82 (25.9%) had hematological neoplasms. The most common cancer diagnosis was breast cancer (n=88, 27.8%) and the most common hematological neoplasm was lymphoma (n=31, 42.5%). On the time of positive PCR for SARS-CoV-2, 220 (69.4%) patients had an active cancer; among those, 170 (77%) had solid malignancies and 50 (23%) had haematological neoplasms. Of the 97 (30.6%) patients who were in remission, 65 (67%) had solid tumors, whereas 32 (33%) had hematological neoplasm. Patients’ characteristics are detailed in Table 1.
Survival outcomes
During the study period, 101(31.9%) patients were hospitalized, 17 (5.3%) were admitted to ICU and 50 (15.8%) have died. The six-month survival rate for the entire cohort was 84.2% (Figure 1). The mortality rate at one month was 14.7%. Notably, in patients who required hospitalization and ICU admission, 42 (41.6%) and 15 (88.2%) died during the hospitalization, respectively.
Overall survial in all patients
Compared to patients who stayed alive, the group of patients who died within six months of COVID-19 infection had a higher frequency of male gender (p=0.018), age > 60 years (p=0.001), diabetes (p=0.008), hypertension (p=0.005), chronic kidney disease (p≤0.001), hematological neoplasms (p=0.005), abnormal serum aspartate aminotransferase (AST) (p=0.038), low albumin (p≤0.001), hemoglobin < 11 g/dl (p=0.017), leucocytosis (p≤0.001) and lymphocyte count <500 (0.004) (Table 2).
On multivariate analysis, low albumin (p≤0.001) and leucocytosis (p≤0.001) correlated with mortality within six months of COVID-19 infection (Table 3).
In the group of patients with active cancer (n=220), the six-month survival rate was 83.1%. In this group, patients who died within six months of COVID-19 infection, compared to survivors, were more likely to be males (p=0.04); older than 60 years (p=0.01); and have hypertension hypertension (p=0.023), chronic kidney disease (p=0.019), hematological neoplasms (p≤0.001), low albumin (p≤0.001), hemoglobin < 10 g/dl (p=0.017), leucocytosis (p≤0.001), lymphocyte count < 500/µl (p=0.004); and have not received recent SACT (p=0.01) (Table 4).
On multivariate analysis, hypertension (p=0.024), no recent SACT (p=0.017), hematological malignancy (p=0.029), low albumin (p≤0.001), leucocytosis (p=0.002) and lymphocyte count < 500/µl (p=0.004), correlated with mortality within six months of COVID-19 infection (Table 5).
Effect of recent administration of SACT
In patients with active cancer (n=220), 99 (45%) received SACT within four weeks of COVID-19 infection. Types of SACT were chemotherapy in 64 (29%), chemoimmunotherapy in 16 (7.2%), immunotherapy in 12 (5.4%), target therapy and hormonal therapy in 5 (2.2%) and 2 (0.9%) patients, respectively. Compared to patients with no recent SACT, patients who received recent SACT had better six-month survival rates (78.8% vs 89.9%, p=0.012), figure (2).
Overall survival in patients with active cancer according to recent SACTSACT: Systemic anticancer treatment
In patients with hematological neoplasm (n=50), the six-month survival rates were comparable between the two groups (64.5% vs 72%, p=0.519), bur in patients with solid tumours, the six-month survival rate was superior in patients who received recent SACT compared to patients who did not (95.9% vs. 82.2%; p=0.006).
We also evaluated the effect of different types of SACT on survival. The 6-month survival rate was inferior in patients who did not receive recent SACT compared to patients who received recent chemotherapy (78.8% vs. 95% %, p=0.04) (Figure 3). However, there was no significant difference in the six-month survival rates between patients who received chemoimmunotherapy and those who did not receive recent SACT (75% vs. 78.8%, respectively; p=0.747).
Overall survival in patients with active cancer according to recent systemic chemotherapy compared to patients with no recent SACTSACT: Systemic anticancer treatment
Impact of COVID-19 infection on the administration of SACT
Among patients with active cancer (n= 220), timely administration of SACT was affected in 140 (63.6%) patients because of COVID-19 infection. SACT was delayed in 105 (47.7%) patients and permanently discontinued in 35 (15.9%) patients.
In 50 patients who had an active hematological neoplasm, SACT administration was delayed in 28 (56%) and permanently discontinued in 13 (26%). The delay was because of hospitalization in 15 (53.6%) patients and due to positive PCR in the remaining patients.
On the other hand, in patients with active solid cancers (n=170), SACT administration was delayed in 77 (45.3%) and permanently discontinued in 22 (12.9%). The delay was because of hospitalization in 17 (22.1%) patients and due to positive PCR in the remaining patients.
Discussion
The COVID-19 pandemic has had profound effects on healthcare services worldwide, and Jordan is no exception. Cancer, a complex group of diseases, relies on timely diagnosis, intervention, and treatment for better prognosis. However, cancer patients, already with weakened immunity, face heightened risks of infectious morbidities. In this study, we explore the impact of the pandemic on cancer patients within the context of limited resources and the unavailability of COVID-19-directed antiviral and antibody treatments.
The overall mortality rate in our study (15.8%) is comparatively lower than the 28% reported by the United Kingdom Coronavirus Cancer Monitoring Project (UKCCMP) study [7]. Notably, our study included all patients (out-patients and hospitalized patients) with a positive PCR test, diverging from the UKCCMP study that focused solely on hospitalized patients. However, the mortality rate among hospitalized patients (41.6%) was higher in our study compared to the UKCCMP study and the Lean European Open Survey on SARS-CoV-2 Infected Patients (LEOSS) registry data [16]. This discrepancy may stem from differing admission criteria and the relative lack of supportive healthcare resources in our setting.
An important observation is the variation in factors independently correlating with mortality between patients with active cancer and the entire patient cohort. While leucocytosis and hypoalbuminemia were independent correlates in the overall patient group, patients with active cancer exhibited independent correlations with other variables, including the diagnosis of hematological neoplasms, lymphopenia and hypertension. It has been reported that COVID-19 immunological signature and post-viral clearance immune state are similar between patients with solid tumors and non-cancer patients [17]. On the other hand, patients with hematological cancer have an exhausted immune response to COVID-19 infection due to lower CD8+ve T cells and B cell aplasia [12]. This may explain the higher impact of impaired immunity on the outcomes in this group.
A significant challenge during the pandemic is the timely administration of SACT. This decision must consider infection severity, cancer type, and treatment goals. Interestingly, we observed a higher six-month mortality rate among patients who did not receive recent SACT. Our findings align with data from the Memorial Sloan Kettering Cancer Centre and the recent UKCCMP study, which also demonstrated that recent chemotherapy was associated with improved six-month survival rates in patients with active cancer and solid tumors [11,12]. Changes in the practice during the pandemic may have resulted in the selection of fitter patients and those being treated with the curative intention to continue SACT. On the other hand, recent SACT was reported to be associated with higher mortality rates in COVID-19-infected cancer patients [9,10]. Notably, this reduction in mortality rates with SACT was not observed in patients with hematologic malignancies, highlighting the need for personalized decision-making based on multiple factors.
The pandemic's impact on the administration of SACT, as reported in our study, is consistent with previous findings [17-20]. Delays in chemotherapy administration, as high as 65% in one study, and delays in chemotherapy, radiotherapy, or surgery in 29-44% of patients in another study, emphasize the challenges faced by cancer patients [19,21]. Patient involvement in critical decisions, as seen in a survey among cancer patients in Lebanon, underscores the importance of considering patients' preferences [22].
Since its discovery in December 2019, several treatments have been approved for managing COVID-19 infections, demonstrating efficacy in cancer patients. In May 2020, remdesivir became the inaugural antiviral agent sanctioned for treating severe COVID-19 infections [23]. A study involving 222 patients with active cancer revealed an 80% reduction in mortality associated with the early use of remdesivir [24]. Neutralizing antibodies, bamlanivimab and etesevimab, targeting the SARS-CoV-2 surface spike glycoprotein, were isolated from convalescent plasma, resulting in decreased hospitalization and mortality rates among high-risk ambulatory patients [25]. Bamlanivimab was particularly effective in reducing hospital and ICU admissions and preventing hypoxia in cancer patients with mild-to-moderate COVID-19 infections [26]. Nirmatrelvir plus ritonavir (Paxlovid) demonstrated an 89% reduction in progression to severe COVID-19 infections in high-risk patients during the Evaluation of Protease Inhibition for Covid-19 in High-Risk Patients (EPIC-HR) trial [27]. A report from the EPICCOVIDEHA registry indicated that COVID-19 patients with hematological malignancies treated with Paxlovid had a lower 30-day mortality (2% vs. 11%) compared to other COVID-19-directed treatments [28]. In the phase 3 component of the MOVe-OUT placebo-controlled trial, oral molnupiravir reduced the risk of hospitalization and death in high-risk patients with mild-to-moderate COVID-19 infections [29]. A matched retrospective study found the efficacy of molnupiravir comparable to Paxlovid in immunocompromised cancer patients [30].
While vaccination remains the paramount and effective preventive measure against SARS-CoV-2 infection, observational studies suggest a potentially blunted serological response to vaccines in cancer patients. This is primarily attributed to the immunosuppressive state of the cancer type and acquired immunodeficiency from anticancer treatments [31,32]. Nevertheless, vaccination is strongly recommended in this group, offering partial protection by inducing long-term T-cell-mediated immunity, irrespective of antibody titers, thereby reducing the risk of breakthrough infections, severe diseases, and hospitalization [33]. Among cancer patients, the mRNA 1237 vaccine appears to be the most immunogenic, followed by BNT162b2 and Ad26.COV2.S [34]. For those with lower antibody titers after the initial vaccine dose, an additional dose may be necessary to enhance immunogenicity [33,34].
Despite being one of the few reports addressing the outcomes and impacts of the COVID-19 pandemic on cancer patients in low- and middle-income countries, we acknowledge the limitations of our retrospective design and the relatively short follow-up time.
Conclusions
COVID-19 infections in our cancer patients resulted in significant morbidity and mortality, negatively impacting the administration of SACT. Recent chemotherapy administration was associated with lower mortality in patients with solid tumors but did not affect the survival of patients with hematological neoplasms. Decisions to delay the administration of SACT in the context of future pandemics should approached with careful consideration.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention JAMA Wu Z Mc Googan JM 1239124232320203209153310.1001/jama.2020.2648 · doi ↗ · pubmed ↗
- 2Number of COVID-19 cases reported to WHO 5 2023 https://data.who.int/dashboards/covid 19/cases?n=c
- 3Prevalence of comorbidities and its effects in patients infected with SARS-Co V-2: a systematic review and meta-analysis Int J Infect Dis Yang J Zheng Y Gou X 91959420203217357410.1016/j.ijid.2020.03.017PMC 7194638 · doi ↗ · pubmed ↗
- 4Patients with cancer appear more vulnerable to SARS-Co V-2: a multicenter study during the COVID-19 outbreak Cancer Discov Dai M Liu D Liu M 7837911020203234559410.1158/2159-8290.CD-20-0422 PMC 7309152 · doi ↗ · pubmed ↗
- 5Impact of cancer diagnoses on the outcomes of patients with COVID-19: a systematic review and meta-analysis BMJ Open Han S Zhuang Q Chiang J 012202210.1136/bmjopen-2020-044661 PMC 882254335131810 · doi ↗ · pubmed ↗
- 6COVID-19 prevalence and mortality in patients with cancer and the effect of primary tumour subtype and patient demographics: a prospective cohort study Lancet Oncol Lee LY Cazier JB Starkey T 130913162120203285355710.1016/S 1470-2045(20)30442-3PMC 7444972 · doi ↗ · pubmed ↗
- 7COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: a prospective cohort study Lancet Lee LY Cazier JB Angelis V 1919192639520203247368210.1016/S 0140-6736(20)31173-9PMC 7255715 · doi ↗ · pubmed ↗
- 8Analysis of the susceptibility of lung cancer patients to SARS-Co V-2 infection Mol Cancer Kong Q Xiang Z Wu Y Gu Y Guo J Geng F 801920203234532810.1186/s 12943-020-01209-2PMC 7186321 · doi ↗ · pubmed ↗