Predictive Role of Preoperative Whole-Body 18F-FDG PET/CT for Risk Stratification of Early-Stage (FIGO I-IIA) Cervical Cancer Patients Treated by Surgery
Nagesh Kumar Singaram, Narendra Hulikal, Ranadheer Manthri, Amith Kumar Chowhan

TL;DR
This study examines how preoperative 18F-FDG PET/CT scans can help predict cancer risk in early-stage cervical cancer patients undergoing surgery.
Contribution
The study evaluates the predictive role of SUVmax from 18F-FDG PET/CT for risk stratification in early-stage cervical cancer patients.
Findings
SUVmax was significantly higher in patients with larger tumors, advanced stage, and deeper invasion.
SUVmax did not independently predict survival outcomes in surgically treated early-stage cervical cancer patients.
The study highlights limitations such as small sample size and lack of multi-metabolic parameters.
Abstract
Introduction: The aim of the present study was to investigate the predictive value of maximum standardized uptake value (SUVmax) measured on preoperative 18F-fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography (18F-FDG PET/CT) in International Federation of Gynecology and Obstetrics (FIGO 2009) stage I-IIA cervical cancer patients who were treated with radical hysterectomy. Methods: A total of 47 patients with FIGO stage I-IIA cervical cancer who were evaluated preoperatively with biopsy and 18F-FDG PET/CT followed by radical hysterectomy were included in the study. Correlation between SUVmax and pathological risk factors or survival was studied. Results: The mean SUVmax was significantly higher in patients with large tumor size (≥4 cm), advanced stage (IIA>IB>IA) and depth of invasion >50%. No significant difference was noted in SUVmax between patients with and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
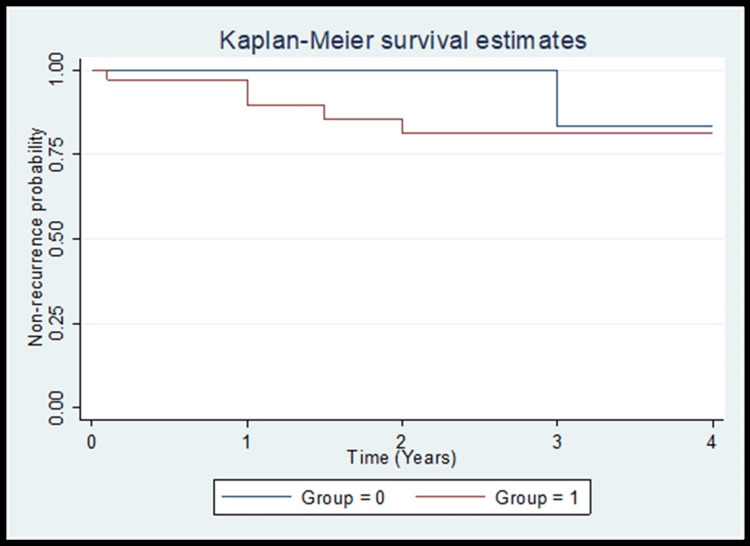 Figure 1
Figure 1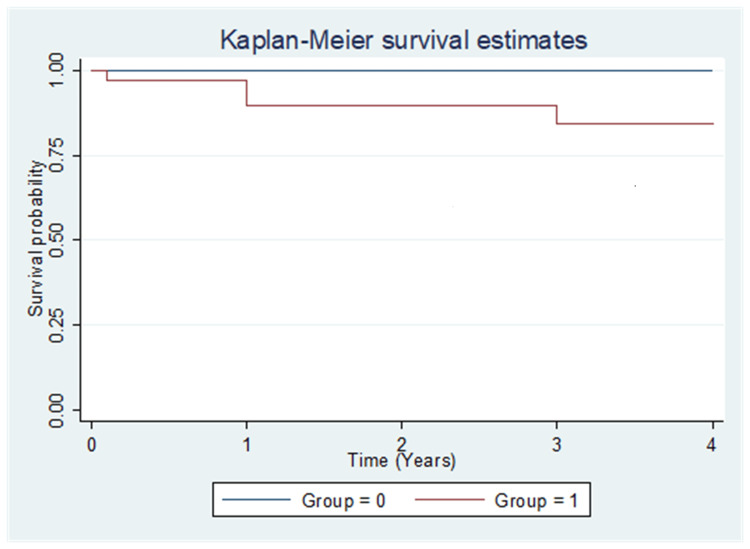 Figure 2
Figure 2| Characteristic | Number | Percentage |
| Total no. of patients | 47 | |
| Mean age at diagnosis | 48.38 ± 11.03 | |
| Initial FIGO stage | ||
| IA1 | 5 | 10.6% |
| IB1 | 11 | 23.4% |
| IB2 | 12 | 25.5% |
| IIA1 | 17 | 36.2% |
| IIA2 | 2 | 4.3% |
| Histopathology | ||
| SCC | 34 | 72.3% |
| AD | 3 | 6.4% |
| Small cell non-keratinizing SCC | 2 | 4.3% |
| Large cell non-keratinizing SCC | 4 | 8.5% |
| ASD | 2 | 4.3% |
| Neuroendocrine carcinoma | 2 | 4.3% |
| Mean size of the tumor | 3.21 ± 1.71 | |
| Median SUVmax (Min–Max) | 11.80 (3.3–40.0) | |
| Pelvic lymph node involvement positive | 3 | 6.4% |
| Median follow-up period in years (Min–Max) | 2.0 (0.0–4.0) | |
| Mean follow-up period (years) | 2.09 (1.44) | |
| Recurrence | 7 | 14.9% |
| Site of recurrence | ||
| Local | 3 | 6.4% |
| Systemic | 4 | 8.5% |
| Death related to cervical cancer | 5 | 10.6% |
| Parametrium | 3 | 6.4% |
| Risk factor for recurrence | SUVmax | P-value |
| Pelvic lymph-node metastasis | 0.639 | |
| Positive | 10.36 ± 6.95 | |
| Negative | 12.28 ± 6.95 | |
| Pathologic tumor size | 0.001 | |
| <4cm | 9.90 ± 5.00 | |
| ≥4cm | 16.54 ± 7.64 | |
| FIGO clinical stage | 0.015 | |
| IA1 | 7.06 ± 3.48 | |
| IB1 | 8.31 ± 5.33 | |
| IB2 | 12.48 ± 4.48 | |
| IIA1 | 15.80 ± 7.86 | |
| IIA2 | 13.25 ± 5.16 | |
| Lymphovascular invasion | ||
| Present | Median SUV 12.95 | 0.5 |
| Absent | 10.35 | |
| Depth of cervical stromal invasion | ||
| <50% | Median SUV 4.7 | 0.003 |
| >50% | 13 |
| SUVmax cutoff | Recurrence rate | P value |
| <7.65 | 8.3% | 0.65 |
| >7.65 | 17.1% |
| Variables | Hazard ratio | 95% CI | p-value |
| Tumor size <4cm | Reference | ||
| Tumor size >=4cm | 2.1 | 0.4 to 10.3 | 0.37 |
| Variables | Hazard ratio | 95% CI | p-value |
| Tumor size <4cm | Reference | ||
| Tumor size >=4cm | 5.9 | 0.6 to 57.1 | 0.09 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometrial and Cervical Cancer Treatments · Ovarian cancer diagnosis and treatment · Endometriosis Research and Treatment
Introduction
Carcinoma cervix is one of the most common malignancies in women with an incidence of 16.5% and mortality rate of 7.5% [1]. Patients with locally advanced and early-stage cervical cancer were treated by chemoradiotherapy and surgery respectively [2-5]. Approximately one fourth of early stage (International Federation of Gynecology and Obstetrics (FIGO) I to IIA) patients develop recurrence. Pathological factors like size, histological type, lymph-vascular space invasion (LVSI), and lymph node status have been used to assess the risk of recurrence [6-9]. Postoperative radiotherapy with or without chemotherapy was given to patients with high risk of recurrence [3,4,9,10]. Selection of patients for adjuvant therapy is important because of its effect on survival and quality of life [4,9]. Identification of independent marker that is associated with biological behavior of cervical cancer is needed along with conventional clinicopathological factors for tailoring the treatment and to avoid dual modality treatment, thereby improving the outcomes in early-stage cervical cancer patients. In many cancers, ^18^F-fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography (^18^F-FDG PET/CT) was used for diagnosis, staging and response assessment [11]. In patients with ovarian cancer and endometrial cancer maximum standardized uptake value ( SUV_max_), measured on ^18^F-FDG PET/CT was found to be useful for diagnosis and prognosis [12-15]. ^18^F-FDG PET/CT has high clinical impact in management of gynecological cancers as it can alter the management plan [16]. The role of ^18^F-FDG PET/CT as a staging tool in cervical cancer was confirmed in previous study [17]. Though the association between SUV_max_ and pathological features of primary tumor has been studied, its prognostic role was not confirmed [18-21]. There is limited evidence on impact of SUV_max_ in early-stage cervical cancer patients treated by surgery [19,20,22]. The present study intends to investigate the predictive role of SUV_max_ measured on preoperative ^18^F-FDG PET/CT for risk stratification of early-stage cervical cancer patients treated by surgery. Primary objective of the study was to assess association between SUV_max_ and recurrence rate or disease-free survival (DFS) or overall survival (OS), secondary objective was to assess the association between SUV_max_ and adverse clinicopathological parameters.
Materials and methods
After approval from the institutional ethics committee (Roc.No.AS/11/IEC/SVIMS/2017, vide IEC No.1462) and informed consent, this prospective study was conducted between June 2018 to June 2019 in the Department of Surgical Oncology, Sri Venkateswara Institute of Medical Sciences, Tirupati, India. A total of 47 biopsy proven early-stage cervical cancer patients (FIGO stage I to IIA) aged between 18 to 80 years who underwent whole body ^18^F-FDG PET/CT followed by surgery (radical hysterectomy) were included. After surgery all pathological risk factors were evaluated and reported by experienced pathologist. Patients with pathological risk factors for recurrence received adjuvant treatment postoperatively. All patients were followed every three months during first two years, then every six months for subsequent two years. Information regarding age; FIGO clinical stage [23]; and clinicopathological features like tumor size, histology type, depth of invasion, LVSI, lymph node metastasis, parametrial involvement and oncological outcomes like recurrence rate, DFS and OS were collected and compared with SUV_max_ which was measured by ^18^F-FDG PET/CT.
Operational definitions: 1) Recurrence - Cancer recurrence was defined as when cancer was found in a patient after completion of treatment and a period in remission had passed; 2) DFS - It was defined as the time from end of treatment to recurrence of tumor or death related to cancer; 3) OS - It referred to the total duration of living time from the end of treatment to death due to any other cause.
Statistical analysis
All data was entered into Microsoft excel sheet. Statistical analysis was done by using SPSS software version 2021.Clinicopathological risk factors and the prognostic data were analyzed for association with the SUV_max_. Cut-off values of the SUV_max_ were determined by the receiver operating characteristic (ROC) curves. Study participants were divided into two groups. Group 0 with SUV_max_ below the cut off value (<7.65) and Group 1 with SUV_max_ above the cut off value (>7.65). Two-sample T test was used to compare the median SUV values in the different subgroups. DFS was calculated using the Kaplan-Meier method. The Cox proportional-hazards model was used for the multivariate analyses. Variables shown to be significant (P<0.05) in the univariate analysis were selected for the Cox model. A P-value of less than 0.05 was considered as significant.
Results
The mean age of the study population was 48.38 ± 11.03 years. Of the patients, 10.6%, 23.4%, 25.5%, 36.2% and 4.3% were at FIGO (2009) stages IA, IB1, IB2, IIA1 and IIA2, respectively. Of the 47 patients, squamous cell carcinoma (SCC) was noted in 34 cases. The mean size of the tumor was 3.21 ± 1.71cm. Median SUV_max_ of the tumor was 11.80 (3.3-40). Lymph node involvement was seen in three cases and parametrium involvement was seen in three cases. The clinicopathological characteristics of study population were shown in Table 1.
Association between SUV_max_ and clinicopathological parameters
Association between the SUV_max_ and clinicopathological factors is shown in Table 2. Significant difference in SUV_max_ was observed among the FIGO stage groups (P= 0.015). The mean SUV_max_ was significantly higher in patients with large tumor size (≥4 cm) compared to patients with tumor size less than 4 cm (P= 0.01). There was no significant difference in SUV_max_ between patient with positive pelvic nodes and negative pelvic nodes (P=0.639). The SUV_max_ of the tumor showing presence and absence of lymph vascular invasion was 12.95 and 10.35, respectively (P=0.5). The median SUV_max_ of tumors with depth of invasion ≥50% was almost thrice that of tumors with depth of invasion <50% (P=0.003).
Correlation between SUV_max_ and recurrence rate
Correlation between SUV_max_ and recurrence rate is shown in Table 3. Recurrence rate in patients with SUV_max_ <7.65 and SUV_max_ >7.65 were 8.3% and 17.1%, respectively (P=0.65).
Correlation between SUV_max_ and DFS
Correlation between SUV_max_ and DFS is shown in Figure 1. There was no difference in DFS between two groups (Group 0 with SUV_max_ <7.65 and Group 1 with SUV_max_ >7.65).
DFS in two groups with lower and higher SUVmax (cut-off value 7.65)Figure1: Group 0 indicates SUVmax < 7.65 and Group 1 indicates SUVmax >7.65.The difference between the two groups was statistically not significant (P=0.3, Log-rank test)SUV: Standardized uptake value; DFS: Disease-free survival
Correlation between SUV_max_ and OS
Correlation between SUV_max_ and OS is shown in Figure 2. There was no difference in OS between two groups (Group 0 with SUV_max <7.65 and Group 1with SUV_max >7.65; P=0.23).
OS between two groups with low and high SUVmax (cut-off value 7.65)Figure 2: Group 0 indicates SUVmax < 7.65 and group 1 indicates SUVmax >7.65.The difference between the two groups was statistically not significant (p=0.23, Log-rank test).SUV: Standardized uptake value; OS: Overall survival
Association of tumor size and recurrence
Association between tumor size and recurrence is shown in Table 4. Patients with tumor size >4cm had 2.1 times high probability of recurrence compared to tumor size <4cm, though not statistically significant (P=0.37).
Table 4: Hazard ratio for recurrence between the groups with tumor size <4cm and >4cm
Association between tumor size and mortality
Association between tumor size and mortality is shown in Table 5. Patients with tumor size >4cm had 5.9 times more probability of mortality compared to tumor size <4cm (P=0.09).
Table 5: Hazard ratio for mortality between the groups with tumor size <4cm and >4cm
Discussion
There were conflicting results regarding predictive and prognostic role of SUV_max_ in cervical cancer patients (FIGO stage I-IV) treated by surgery, radiotherapy or palliative treatment [18,19]. These different results may be due to treatment bias as disease stages and treatment modalities were different. In early stage (IA-IIA) cervical cancer treated exclusively with surgery, there have been controversial studies on the role of SUV_max_, Lee et al. showed impaired DFS was correlated with high SUV_max_, while Crivellaro et al. showed increased recurrence was not associated with SUV_max_[19,21]. To clarify the predictive value of SUV_max_ the present study focused on FIGO stage IA -IIA who were only treated by surgery as primary modality. In present study, there was statistically significant difference between median SUV_max_ and FIGO stages, lower and higher stage tumor had lower and higher SUV_max_ respectively. Present study results are in concordance with study by Chung et al. that reported that higher FIGO stages are associated with high SUV_max_ (P =0.01) [22]. In contrast, Yu et al. reported that no statistical significance between groups with stage IB and IIA diseases in relation to SUV_max (P > .05) [24]. In a study done by Yagi et al., SUV_max of the primary tumor on preoperative ^18^F-FDG-PET/CT was a prognostic indicator in patients with stage IA2 to IIB cervical cancer treated with radical hysterectomy [25].
Present study showed that a high SUV_max_ of primary tumor was significantly correlated with presence of conventional adverse clinicopathological risk factors such as tumor size, depth of cervical stromal invasion. In the present study, the median SUV_max_ of tumor <4cm and > 4cm was 9.7 and 13.6, respectively, which was comparable with study done by Xu et al., in which <4cm tumor SUV_max was 9.77 and tumor > 4cm the SUV_max was 14.86 [26]. In present study and study done by Xu et al., there was statistically significant difference between the two groups, which means higher SUV_max_ correlates with large size tumor. In the present study, the median SUV of tumor in patients with cervical stromal depth of invasion>50% was 13, which was comparable with studies done by Xu et al. (12.44) and Zhang et al. [26,27]. Further, in these studies and the present study, there was statistically significant difference in SUV_max between the two groups. Cut-off values of SUV_max for predicting lymph node metastasis was 6.03, cut-off for OS and DFS were 7.36 and 5.59, respectively, in all stages (IA-IIA). Consistent with present results, the study by Yun et al. showed that the cut off value of SUV_max_ >6 was predictive of DFS in stage IA-IIA [28]. In contrast, Lee et al. reported higher cut-off value (SUV_max_>13.4), which was predictive disease recurrence in stage IB1-IIA [19]. The study by Kidd et al. observed three subgroups according to the SUV_max_ cut off values low (<5.2), middle (5.2-13.3), and high (>13.3) [18]. Among these studies the cut-off values of SUV_max_ are different it can be due to ^18^F-FDG PET/CT settings, image analysis, condition of patient, and stage of disease.
In the present study, we did not find any significant differences in recurrence rate, DFS and OS among the two groups group with SUV_max_ <7.65 and SUV_max_ >7.65. Our findings are in concordance with study done by Crivellaro et al. [21]. In contrast, our findings are not in concordance with study done by Lee et al., who reported that in early-stage cervical cancer, tumors with high SUV_max_ (≥13.4) are at increased risk of recurrence [19].
In this study, the hazard ratio for mortality was 5.9 times higher in tumors >4cm compared to tumors <4cm (P=0.09), which is in concordance with study done by Wagner et al. that reported that with inclusion of size >4 cm for stage IIA cancers in new FIGO staging system for cervical cancer, it was better correlated with survival and overall prognosis [29]. Also, a study done by Kyung et al. reported that tumor size (4 vs 4-6 cm, P=.0371; and 4 vs >6 cm, P=.0024) was an independent predictive factor for the prognosis of stage II to IV cervical cancer [30].
Limitations
Other parameters of ^18^F-FDG PET/CT like metabolic tumor volume (MTV) and tumor lysis glycolysis (TLG) were not used along with SUV_max_ for prognostication in this study. Small sample size, variation in calculation of SUV_max_, histopathologic heterogeneity, and inclusion of stage IA patients in the study were some of the limitations observed in our study. Further studies using multi metabolic parameters of ^18^F-FDG PET/CT, including SUV_max_, SUV_mean_, SUV_peak_, MTV, and TLG are needed.
Conclusions
SUV_max_ on preoperative whole body ^18^F-FDG PET/CT can be used to differentiate between stage I and II cancer and to predict unfavorable clinicopathological features in FIGO stage IA-IIA patients who have undergone radical hysterectomy. These findings suggest that the SUV_max_ of the primary tumour may be a promising marker for risk stratification in surgically treated, early-stage invasive cervical cancer patients. The present study did not find any difference in long term oncological outcomes between the groups; however, it showed higher hazard of recurrence and mortality in patients with tumor size > 4cm, which in turn correlated with higher SUV_max_. Future studies with large sample size and inclusion of other ^18^F-FDG PET/CT parameters along with SUV_max_ may throw light on their prognostic significance and individualizing treatment in early stage (IA2-IIA2) cervical cancer patients undergoing radical hysterectomy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin Bray F Ferlay J Soerjomataram I Siegel RL Torre LA Jemal A 3944246820183020759310.3322/caac.21492 · doi ↗ · pubmed ↗
- 2Multimodality therapy for locally advanced cervical carcinoma: state of the art and future directions J Clin Oncol Monk BJ Tewari KS Koh WJ 295229652520071761752710.1200/JCO.2007.10.8324 · doi ↗ · pubmed ↗
- 3Annual report of the Committee on Gynecologic Oncology, the Japan Society of Obstetrics and Gynecology J Obstet Gynaecol Res Yamagami W Aoki D 186118694120152642074610.1111/jog.12833 · doi ↗ · pubmed ↗
- 4Reconsideration of postoperative concurrent chemoradiotherapy with fluorouracil and cisplatin for uterine cervical cancer J Obstet Gynaecol Res Takekuma M Kasamatsu Y Kado N 163816434120152617779010.1111/jog.12754 · doi ↗ · pubmed ↗
- 5Multivariate analysis of histopathologic prognostic factors for invasive cervical cancer treated with radical hysterectomy and systematic retroperitoneal lymphadenectomy Acta Obstet Gynecol Scand Takeda N Sakuragi N Takeda M 114411518120021251911110.1034/j.1600-0412.2002.811208.x · doi ↗ · pubmed ↗
- 6Histopathologic parameters of prognosis in cervical cancer-a review Int J Gynecol Cancer Singh N Arif S 7417501420041536118010.1111/j.1048-891X.2004.014504.x · doi ↗ · pubmed ↗
- 7Radical hysterectomy for FIGO stage I-IIB adenocarcinoma of the uterine cervix Br J Cancer Kasamatsu T Onda T Sawada M Kato T Ikeda S Sasajima Y Tsuda H 1400140510020091940169910.1038/sj.bjc.6605048 PMC 2694432 · doi ↗ · pubmed ↗
- 8Clinicopathologic factors of cervical adenocarcinoma stages IB to IIB Int J Gynecol Cancer Mabuchi Y Yahata T Kobayashi A 167716822520152649576010.1097/IGC.0000000000000542 · doi ↗ · pubmed ↗